51 Noninvasive Positive-Pressure Ventilation
Noninvasive ventilation is defined as the provision of ventilatory assistance to the lungs without an invasive artificial airway. Noninvasive ventilators consist of a variety of devices, including negative- and positive-pressure ventilators. Until the early 1960s, negative-pressure ventilation in the form of tank ventilators was the most common type of mechanical ventilation outside the anesthesia suite.1 However, during the Copenhagen polio epidemic of 1952, it was observed that the survival rate improved when patients with respiratory paralysis were treated with invasive positive-pressure anesthesia devices. After that, invasive positive-pressure mechanical ventilation gradually became the preferred means of treating acute respiratory failure.2 Negative-pressure and other so-called body ventilators were the mainstay of ventilatory support for patients with chronic respiratory failure until the mid-1980s.1
With improving mask and ventilator technology and the many advantages over negative-pressure ventilation,1 noninvasive positive-pressure ventilation (NIPPV) displaced negative-pressure ventilation as the treatment of choice for chronic respiratory failure in patients with neuromuscular and chest wall deformities.3 Over the past 15 years, noninvasive ventilation has moved from the outpatient to the inpatient setting, where it is used to treat acute respiratory failure. A 1997 survey of medical intensive care units (ICUs) in France, Switzerland, and Spain demonstrated that noninvasive ventilation was used in 16% of cases in which mechanical ventilation was required for respiratory failure, and a follow-up survey found that this rate was up to 23% in 2001.4 More recent surveys suggest that rates continue to increase over these levels.5 This chapter discusses the rationale for the increasing use of NIPPV in critical care, as well as appropriate indications, practical applications, and monitoring.
 Rationale
Rationale
The most important advantage of noninvasive ventilation is the avoidance of complications associated with invasive mechanical ventilation. These include complications related to direct upper-airway trauma, bypass of the upper-airway defense mechanisms, increased risk of nosocomial pneumonia, and interference with upper-airway functions, including the ability to eat and communicate normally.6 By averting airway intubation, noninvasive ventilation leaves the upper airway intact, preserves airway defenses, and allows patients to eat orally, vocalize normally, and expectorate secretions. Compared with invasive mechanical ventilation, noninvasive ventilation reduces infectious complications including pneumonia, sinusitis, and sepsis.7–9 Strengthening the rationale for its use is evidence accumulated over the past decade that noninvasive ventilation lowers morbidity and mortality rates of selected patients with acute respiratory failure and may shorten hospital length of stay or avoid hospitalization altogether,10 thus reducing costs.
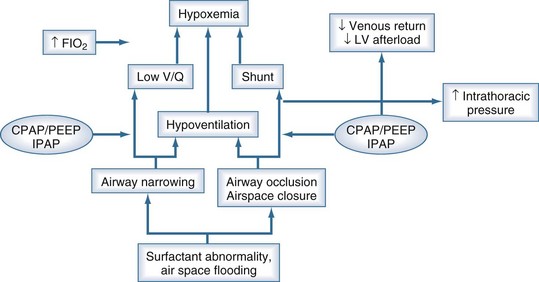
The main indication for mechanical ventilatory assistance is to treat respiratory failure, either type 1 (hypoxemic), type 2 (hypercapnic), or both. Figure 51-1 shows that airspace collapse, surfactant abnormalities, and airway narrowing and closure contribute to ventilation-perfusion abnormalities and shunt, which cause hypoxemia. By opening collapsed airspaces and narrowed airways, positive airway pressure reduces shunt and improves ventilation-perfusion relationships, ameliorating hypoxemia. In addition, positive airway pressure can reduce the work of breathing by improving lung compliance as a consequence of opening collapsed airspaces. Another potential benefit of positive airway pressure is enhanced cardiovascular function via the afterload-reducing effect of increased intrathoracic pressure. Conversely, deleterious cardiovascular effects may occur if the preload-reducing effect outweighs the afterload-reducing effect, as may be seen in patients with reduced intravascular fluid volume.
 Mechanisms of Action
Mechanisms of Action
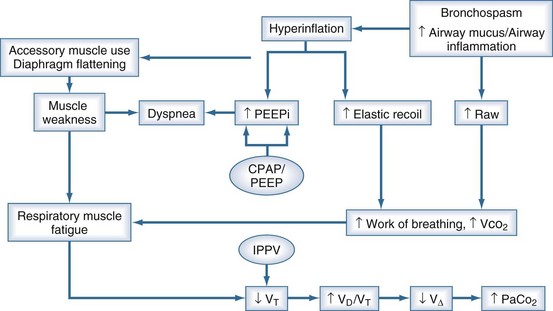
Figure 51-2 shows the pathophysiologic mechanisms that contribute to ventilatory failure. Increased airway resistance, reduced respiratory system compliance, and intrinsic positive end-expiratory pressure (PEEP) contribute to increased work of breathing, predisposing to respiratory muscle fatigue. In patients with chronic obstructive pulmonary disease (COPD), the increased radius of the diaphragmatic curvature, which increases muscle tension and thereby increases impedance to blood flow, exacerbates the situation. By counterbalancing intrinsic PEEP with extrinsic PEEP and by augmenting tidal volume with intermittent positive-pressure ventilation, NIPPV reduces the work of breathing and averts the vicious circle leading to respiratory failure. Work of breathing measurements, including transdiaphragmatic pressure, diaphragmatic pressure-time product, and diaphragmatic electromyographic amplitude, are all decreased when NIPPV is delivered to patients with exacerbations of COPD. In such patients, continuous positive airway pressure (CPAP) and pressure-support ventilation (PSV) both reduce the work of breathing, but the combination of the two (PSV + PEEP) is more effective than either alone.11
 Indications
Indications
A number of causes of acute respiratory failure are now considered appropriate for noninvasive ventilation therapy and are listed in Box 51-1. Evidence supporting these indications is rated and briefly discussed here; guidelines for patient selection are discussed later.
Box 51-1
Indications for Use of Noninvasive Ventilation in the Acute Care Setting
Airway Obstruction
Chronic Obstructive Pulmonary Disease
A number of randomized controlled trials12,13 and meta-analyses14 have consistently shown that compared with conventional therapy, NIPPV improves vital signs, gas exchange, and dyspnea scores; reduces the rates of intubation, morbidity, and mortality; and shortens hospital length of stay in patients with moderate to severe exacerbations of COPD. Thus NIPPV is considered the ventilatory mode of choice in selected patients with acute exacerbations of COPD. Some studies suggest that the addition of heliox to NIPPV further improves the work of breathing and gas exchange during COPD exacerbations,15 but a subsequent multicenter trial found no improvement in other outcomes compared with noninvasive ventilation alone.16
Asthma
Uncontrolled studies have reported improvements in gas exchange and low rates of intubation after the initiation of NIPPV in patients with severe asthma attacks. Two controlled trials have demonstrated a more rapid improvement in expiratory flow rates with NIPPV,17,18 and one showed a decreased hospitalization rate in acute asthma patients treated with noninvasive ventilation compared with a sham mask.18 Neither study was powered adequately to assess intubation or mortality rates. Nonetheless, these data support a trial of NIPPV in asthmatics responding poorly to initial bronchodilator therapy. Noninvasive ventilation can be combined with continuous nebulization and heliox, although the added value of these latter therapies has not been established in controlled trials.
Cystic Fibrosis
Uncontrolled studies indicate that noninvasive ventilation is useful to stabilize gas exchange in the treatment of acute episodes of respiratory failure in end-stage cystic fibrosis patients and can serve as a bridge to transplantation.19
Hypoxemic Respiratory Failure
Hypoxemic respiratory failure is defined as severe hypoxemia (arterial oxygen partial pressure-inspired oxygen fraction ratio <200) combined with a respiratory rate above 35 breaths per minute and a non-COPD diagnosis including acute pneumonia, acute lung injury (ALI), acute respiratory distress syndrome (ARDS), pulmonary edema, or trauma. Controlled trials of noninvasive ventilation to treat patients with acute hypoxemic respiratory failure have shown statistically significant reductions in the rate of intubation, length of hospital stay, incidence of infectious complications,8,20 and in one study, ICU mortality.20 However, because of the heterogeneity of causes, these studies fail to demonstrate that all patient subgroups with hypoxemic respiratory failure benefit equally from noninvasive ventilation. Further, when patients are stratified according to acuity of illness, patients with a simplified acute physiologic score (SAPS II) less than 35 fare considerably better with NIPPV than do those with higher scores.21 Thus the selection of patients with less severe disease is likely to enhance the success of NIPPV in treating hypoxemic respiratory failure, and studies that examine individual subgroups within the larger category are likely to be more useful clinically.
Pneumonia
One controlled trial showed that noninvasive ventilation in patients with severe community-acquired pneumonia lowers the rate of endotracheal intubation and shortens the length of ICU stay compared with conventional therapy; however, a subgroup analysis revealed that the benefits occurred only in patients with underlying COPD.22 No benefit was apparent in the non-COPD patients with severe pneumonia. A subsequent uncontrolled trial in non-COPD patients with severe pneumonia found that two-thirds of such patients treated with noninvasive ventilation eventually required intubation.23 Although the latter authors deemed a trial of noninvasive ventilation in non-COPD patients with severe pneumonia to be a reasonable approach, controlled data to support such a recommendation are currently lacking.
Immunocompromised States
The dismal prognosis of invasively ventilated immunocompromised patients makes noninvasive ventilation an appealing ventilatory mode, with its demonstrated ability to decrease the rate of nosocomial infection.7 In a study of 51 patients undergoing solid organ transplantation who developed acute hypoxemic respiratory failure within 3 weeks, noninvasive ventilation reduced the rate of intubation, frequency of invasive procedures, rate of nosocomial infection, duration of ICU stay, and ICU mortality (but not hospital mortality) compared with conventional therapy.24 In a subsequent randomized trial of neutropenic patients with pulmonary infiltrates and acute hypoxemic respiratory failure (most of whom had hematologic malignancies), noninvasive ventilation lowered the intubation rate, occurrence of nosocomial infections, and ICU and hospital mortality rates (the latter from 80% to 46%).25 More recently, noninvasive ventilation has been reported to yield similar benefits in acquired immunodeficiency syndrome (AIDS) patients with Pneumocystis carinii pneumonia versus invasive mechanical ventilation in physiologically and demographically matched patients.26 Thus, whenever possible, noninvasive ventilation should be tried first in immunocompromised patients with hypoxemic respiratory failure because of the potential to avoid the high morbidity and mortality rates associated with invasive mechanical ventilation in these patients.
Acute Respiratory Distress Syndrome
A small retrospective study reported that NIPPV averted intubation in 50% of patients during the early phase of acute lung injury or ARDS.27 However, for ARDS patients with severe oxygenation defects and multiple organ system dysfunction, invasive ventilation remains the preferred modality. A prospective cohort study28 using noninvasive ventilation as a “first-line” intervention for ARDS found that ventilator associated pneumonia and mortality were much reduced when patients succeeded rather than failed noninvasive ventilation, and a simplified acute physiology score of 34 or less and PAO2/FIO2 above 175 within the first hour predicted noninvasive ventilation success. Thus, noninvasive ventilation could be considered in ARDS patients meeting these criteria, but such patients must be monitored closely to avoid any delay in intubation if deterioration occurs.
Acute Cardiogenic Pulmonary Edema
Meta-analyses of randomized, controlled trials demonstrated that compared with oxygen therapy, CPAP (though not a true mode of ventilatory support) is highly effective at relieving respiratory distress, improving gas exchange, and averting intubation when used to treat patients with acute cardiogenic edema.29,30 Inspiratory assistance combined with expiratory pressure can reduce the work of breathing and alleviate respiratory distress more effectively than CPAP alone, and several uncontrolled trials and two controlled trials found that noninvasive ventilation and CPAP are equally effective in improving vital signs and avoiding intubation. The current recommendation is to use CPAP alone or noninvasive ventilation as initial therapy; if CPAP is used initially, inspiratory pressure support should be added if the patient has persistent hypercapnia or dyspnea.31
Postoperative Respiratory Failure
NIPPV and CPAP alone have been studied in postoperative patients who develop respiratory failure after various kinds of surgery. It reduces extravascular lung water and improves lung mechanics and gas exchange after coronary artery bypass surgery.32 Controlled trials show that CPAP averts postoperative complications compared to oxygen supplementation after high risk procedures like thoracoabdominal aortic procedures.33 Noninvasive ventilation improves oxygenation, reduces the need for re-intubation, lowers the mortality rate after lung resectional surgery,34 and enhances pulmonary function after gastroplasty.35 Thus noninvasive ventilation should be considered in selected postoperative patients at high risk of pulmonary complications or with frank respiratory failure, especially in the setting of underlying COPD or pulmonary edema.



Full access? Get Clinical Tree


