Noninvasive Blood Pressure Management—It’s Not Just a Piece of Nylon Around the Arm
Jorge Pineda JR MD
Stephen T. Robinson MD
The automated, noninvasive, blood-pressure cuff is a safe, commonly used monitoring device. It provides consistent, reliable values for systolic, diastolic, and mean arterial pressure (MAP). One great advantage of such a monitor is that it frees the anesthesiologist for other tasks. Blood-pressure-cuff cycling intervals can be set and the machine can store data to provide trends. Automated devices also provide alarm systems to draw attention to extremes in blood-pressure values. Disadvantages include frequent failure with profoundly hypotensive patients, patients with arrhythmias, and during periods of movement artifact (resulting, for instance, from shivering or tremors).
OSCILLOMETRY
Most noninvasive devices used in current practice measure blood pressure by oscillometry. In this method, variations in cuff pressure resulting from arterial pulsations during cuff deflation are sensed by the monitor and used to determine pulsations corresponding closely to true mean arterial pressure. The cuff is inflated to a pressure above the previous systolic pressure and then it is deflated incrementally. A transducer senses the pressure changes, which are then processed by the microprocessor. This technique has an accuracy of ±2%. The mean arterial pressure corresponds to the maximum oscillation (maximum amplitude = Amax) at the lowest cuff pressure (Fig. 88.1).
Systolic and diastolic pressure readings are derived indirectly from formulas that examine the rate of change of the pressure pulsations. It has been determined that systolic and diastolic pressure occur when the amplitudes of oscillation (Asystolic and Adiastolic) are a certain fraction of Amax. The systolic pressure corresponds to the onset of rapidly increasing oscillations. Algorithms used by different manufacturers vary and are never publicly disclosed, making it impossible for investigators to verify the accuracy of their underlying physiologic principals. In general, the systolic pressure is chosen as the pressure above the mean pressure at which oscillations are increasing in amplitude and are at 25% to 50% of the maximum (Asystolic/Amax = 0.25 to 0.5). Diastolic pressure corresponds to the onset of rapidly decreasing oscillations and is more difficult to determine. It is commonly labeled as the
point below the mean pressure at which the pulse amplitude has declined to 60% of Amax (Adiastolic/Amax = 0.6), or it is calculated from the systolic and mean arterial pressure, using the following formula: MAP = diastolic + one-third pulse pressure. main problem with this technique is that the amplitude of the oscillations depends on several factors other than blood pressure, such as the stiffness of the arteries. Elderly subjects and patients with “stiff,” atherosclerotic arteries have a loss of arterial wall compliance, which is associated with higher systolic and diastolic blood pressure readings using blood-pressure cuffs as compared with values obtained from direct arterial measurements.
point below the mean pressure at which the pulse amplitude has declined to 60% of Amax (Adiastolic/Amax = 0.6), or it is calculated from the systolic and mean arterial pressure, using the following formula: MAP = diastolic + one-third pulse pressure. main problem with this technique is that the amplitude of the oscillations depends on several factors other than blood pressure, such as the stiffness of the arteries. Elderly subjects and patients with “stiff,” atherosclerotic arteries have a loss of arterial wall compliance, which is associated with higher systolic and diastolic blood pressure readings using blood-pressure cuffs as compared with values obtained from direct arterial measurements.
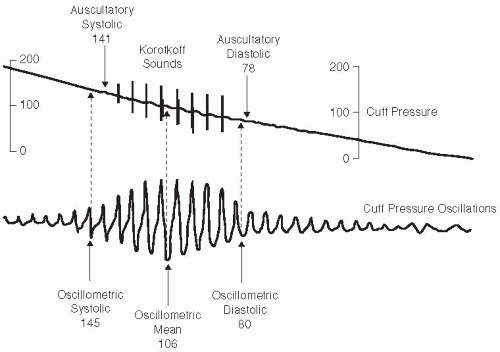 FIGURE 88.1. Blood pressure from Karotkoff sounds (top) compared to oscillometry (bottom). From Geddes LA. Cardiovascular Devices and their Applications. New York: John Wiley; 1984: Fig. 34.2. |
PROPER USE
Related posts:
 Never Neglect the Basics of Airway Management
Consider the Use of Lidocaine in the Cuff of the Endotracheal Tube, But Be Aware of the Risks and Alternatives
Do Not Underestimate the Difficulty of Reintubating a Patient Who Has Undergone Carotid Endarterectomy or Cervical Spine Surgery
Don’t Overflush Lines
Do Not Treat Lactic Acidosis with Bicarbonate
Beware the Antibiotic Bowel Prep
Never Neglect the Basics of Airway Management
Consider the Use of Lidocaine in the Cuff of the Endotracheal Tube, But Be Aware of the Risks and Alternatives
Do Not Underestimate the Difficulty of Reintubating a Patient Who Has Undergone Carotid Endarterectomy or Cervical Spine Surgery
Don’t Overflush Lines
Do Not Treat Lactic Acidosis with Bicarbonate
Beware the Antibiotic Bowel Prep

Full access? Get Clinical Tree


