Neurologic System
Accommodation
Accommodation is the adaptation of eyes for near vision. It is demonstrated by having patient focus on object at arm’s length. When object is brought toward patient, the pupils should converge and constrict. This cannot be done on a comatose patient.
Acoustic Neuroma
(see Tumors, Neurogenic, p. 61)
Adenoma
(see Tumors, Neurogenic, p. 63)
Amyotrophic Lateral Sclerosis
(see also Spinal Cord, p. 53)
ALS, commonly known as Lou Gehrig’s disease, is a chronic progressive neurodegenerative disease of unknown cause that adversely affects the upper and lower motor neurons (wasting and weakness of muscles is related to lower motor damage, whereas spasticity and exaggerated weakness is related to upper motor neuron damage). Over time, motor neuron destruction leads to the inability to innervate and control voluntary muscle fibers. The result is muscle weakness and atrophy with eventual total loss of muscle function leading to respiratory failure and death. The disease does not affect the individual’s sensory or cognitive abilities.
Anatomy: Arterial Blood Supply to Brain
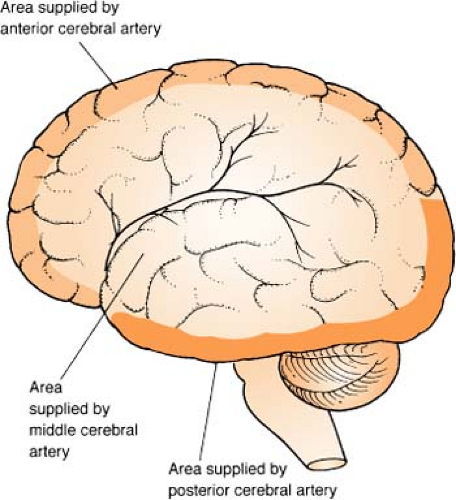 Figure. Arterial blood supply to the brain. |
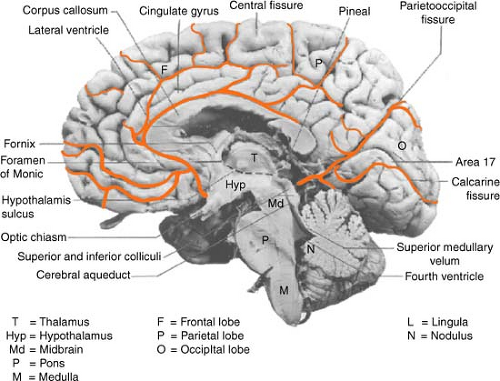 Figure. Major blood vessels to brain. (Used with permission from Hendelman, W. J. [2000]. Atlas of functional neuroanatomy. Boca Raton, FL: CRC Press.) |
Anatomy: Brain Structures and Function
(see also Tumors, Neurogenic, p. 61)
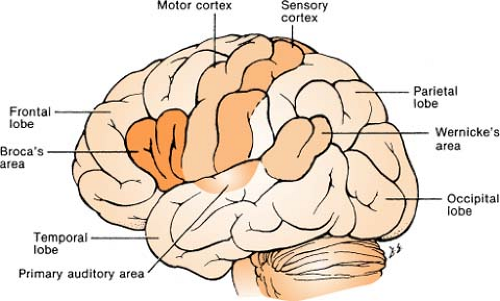 Figure. Cerebrocortical areas involved in communication. |
Frontal
Located in front of skull
Plan for future
Speech
Prefrontal: Controls respiration, gastrointestinal (GI) activity, circulation, pupillary reactions, and emotions; helps regulate personality, thought processes, intellect, math ability, and concentration
Broca’s area: Controls ability to articulate speech. Contained in one hemisphere and is almost always dominant in the left. Damage to this area may cause motor aphasia.
Written speech area: Controls ability to write words. Regardless of whether patient is right or left handed, this area is usually situated in the left cerebral hemisphere.
Parietal
Located up near crown of head
A primary sensory area; receives sensory stimuli from other parts of the body and defines them according to size, shape, weight, texture, consistency, position sense, touch, and pressure.
Processes visual-spatial information in nondominant lobe
Temporal
Located around temples
Second weakest bone in skull
Deals with sound
Wernicke’s area: Works to understand spoken word and written language
Auditory speech: Integrates sound into pitch, quality, and loudness
Postcranial area: Controls body’s sensory areas
Occipital
Located at bottom and back of head
Visual: Integrates visual stimulation for size, form, motion, and color
Corpus Callosum
Located in center of brain
A thick area of nerve fibers connecting one hemisphere to the other
Prevents chaos between hemispheres
Cerebellum
Located at base of cerebrum
Divided into two hemispheres, each composed of gray and white matter; governs walking, balance, coordination, and muscular memory
Remember:
A lesion in the cerebellum presents signs and symptoms (e.g., ataxia) on the same side of the body (the ipsilateral side).
Midbrain
The top part of the brain stem
CN III and CN IV exit here; the pathway for cerebral hemispheres and the center for auditory and visual reflexes
Pons
The middle part of the brain stem
CN V through CN VIII exit here; maintains a bridge between midbrain and medulla
Controls respiratory function
Medulla
The bottom part of the brain stem; attaches to spinal cord
CN IX through CN XII exit here; transmits information for coordination of head and eye movements, and contains cardiac, vasomotor, and respiratory centers
Thalamus
White matter located deep in the center of the brain near the brain stem
Responsible for the sense of movement and position, and the ability to recognize size, shape, and quality of objects
Also responsible for the routing of all sensory stimuli to their destinations, including the cerebral cortex, which receives them and translates them into appropriate responses
Hypothalamus
Located between the pituitary gland and the brain stem
Regulates appetite, sexual arousal, thirst, temperature, hormonal secretions, water metabolism, and visible physical expressions in response to emotions (blushing, clammy hands, dryness of mouth)
Also the center for the autonomic nervous system
Pituitary Gland
Located “front and center” of brain
Considered the “master gland” because of the number of hormones and functions it controls. The pituitary receives the “OK” from the hypothalamus to secrete hormones via the pituitary stalk (infundibulum).
Anterior lobe secretes growth stimulating hormone (GSH), adrenocorticotropin hormone (ACTH), thyroid stimulating hormone (TSH), follicle stimulating hormone (FSH), and luteinizing hormone (LH).
Posterior lobe secretes antidiuretic hormone (ADH) and oxytocin.
Anatomy: Cranial Layers
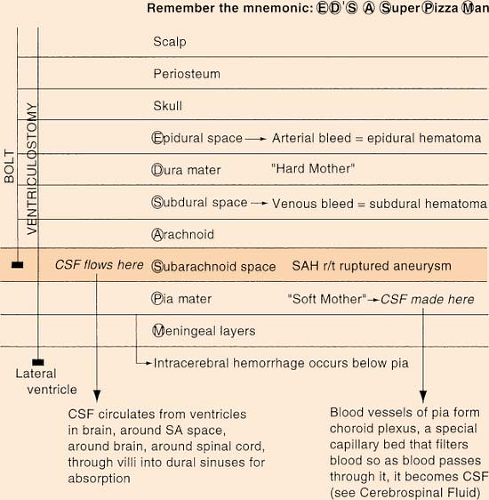 Figure. Cranial layers. |
Aneurysms: Cerebral
(see also Embolization, p. 26; Subarachnoid Hemorrhage, p. 60; Vasospasm, p. 64)
Subarachnoid Grading Scale
Numerous subarachnoid grading scales have been proposed; however, the Hunt and Hess scale is the most widely used (see figure).
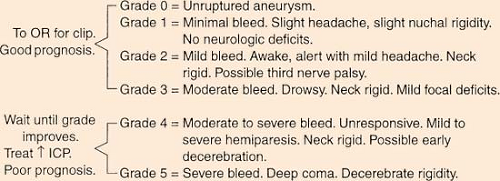 Figure. Hunt and Hess scale. |
Rebleed risk: Peak incidence occurs 24 to 48 hours after initial bleed. Approximately 30% to 40% of patients rebleed within first several weeks, with mortality rate of 42%.
Vasospasm: Occurs in 40% to 60% of all patients with subarachnoid hemorrhage (SAH), usually day 5 to 7 after bleed (not after surgery) but can occur from day 1 to day 21.
Survival: On average, 25% die the first day, and 50% die within the first 3 months; 50% of survivors have major deficits.
Sites: About 85% of aneurysms are located anteriorly. This is good because the posterior area is difficult to access.
Size:
Super giant: >50 mm
Giant: 25 to 50 mm
Large: 15 to 25 mm
Small: <15 mm
Types (see figures):
Berry: Most common. Rounded with a neck or stem, looks like “berries.”
Saccular: Any aneurysm having a saccular outpouching from one wall.
Fusiform: Diffuse enlargement of arterial wall in all directions. No neck or stem; looks like a balloon. Usually does not cause SAH.
Charcot-Bouchard: Origin is basal ganglia or brain stem. Microscopic formations related to hypertension.
Mycotic: Rare; caused by septic emboli that separate endothelial lining; related to bacterial endocarditis.
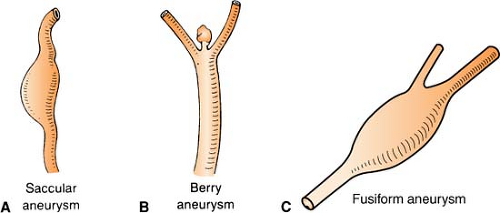 Figure. Saccular, berry, and fusiform aneurysms. (Part C: Adapted from Brain Aneurysm Foundation, Inc., Boston, MA.) |
Surgical intervention: Clipping or ligation of the aneurysm neck provides the best protection against rebleeding, although the initial risk may be slightly higher. Since the early 1990s, some cerebral aneurysms have been treated using embolization (coiling), wherein platinum Guglielmi detachable coils (GDCs) are packed into the aneurysm to prevent blood from flowing into it (see also Embolization).
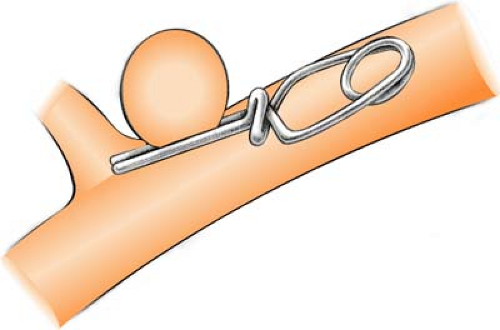 Figure. Clipping a cerebral aneurysm. (From Springhouse. [2008]. Visual nursing. Philadelphia: Lippincott Williams & Wilkins.) |
Embolization: Since the early 1990s, an endovascular technique called “coiling” has also been used. It involves the interventional radiologist guiding a catheter from the femoral artery, up through the aorta, and into the cerebral vasculature, via either the carotid or the vertebral artery, until it reaches the cerebral aneurysm. Tiny platinum coils are then threaded through the catheter into the aneurysm to pack it tightly and close off blood flow into it, thereby preventing rupture. This process is called embolization. The coil itself has a memory effect (similar to a slinky toy) that allows it to form a coil of a given radius, thickness, and softness. Coils are manufactured in a variety of sizes from 2 mm in diameter or more, and in different lengths. They also come in two thicknesses, 10/1000 and 18/1000, and two stiffnesses, soft and regular. Occasionally, it is necessary to put more coils in later to complete treatment.
Angiography, Cerebral
Cerebral angiography is a diagnostic tool that produces images of the blood vessels of the brain with the added benefit of interventional capabilities during the procedure, if required. As with any angiogram, access is gained via the femoral or brachial arteries. A catheter is then threaded through this access to the carotid arteries, where contrast medium is injected directly into the arterial vasculature of the brain (known as “shooting the carotids”). Digital subtraction angiography (DSI) removes bone and tissue from the image, leaving only the dye-filled blood vessels for optimal visualization and interpretation. Postprocedure care includes observance of routine angiogram complications, as well as an added neurological assessment. Complications of this procedure include artery/arterial wall damage or dislodgement of debris such as plaque or a clot, which may result in a stroke.
Apneustic Breathing
(see Respiratory Patterns in Part 3, p. 203)
Arteriovenous Malformation
Arteriovenous malformations (AVMs) are congenital brain lesions composed of tangled, dilated vessels that form an abnormal communication between arterial and venous systems. Intracranial “steal” occurs when the AVM is large, related to blood being diverted from one area of brain tissue because of lower vascularization in another area.
Signs and symptoms: Seizure activity is most common. Hemorrhage and/or headache occurs in about 50% of patients.
Treatment: Similar to aneurysms, though AVMs pose less risk of bleed with intervention.
Embolization
Surgical excision
Gamma knife, linear accelerator, or proton beam radiation (for surgically inaccessible AVMs)
 Figure. Arteriovenous malformation. (Courtesy of UT Southwestern University Hospital—Zale Lipshy, Dallas, Texas.) |
Astrocytoma
(see Tumors, Neurogenic, p. 62)
Autonomic Dysreflexia
(see Dysreflexia, p. 24)
BABINSKI’s REFLEX
Positive response for Babinski’s reflex is fanning of toes and extension of great toe with stimulation of plantar surface of foot. It is normal in babies but abnormal in adults. Response is related to upper motor neuron lesion and is seen on opposite side of cerebral damage.
Negative response is flexion of foot and is normal in adults.
Basilar Skull Fracture
Injury to the olfactory (first cranial) nerve is common with fracture, along with otorrhea or rhinorrhea. Drainage sample may be positive for glucose, though this is not always a reliable sign. Allow cerebrospinal fluid (CSF) to drain freely, keeping in mind that draining CSF due to a torn dura puts the patient at high risk for meningitis. Avoid NG, nasal suction, Valsalva’s maneuver, and cough. Raccoon eyes (ecchymotic areas around the eye orbits), epistaxis, visual defects, and anosmia are indicative of anterior fossa fracture, whereas Battle’s sign (ecchymosis over the mastoid bone 24 to 48 hours after injury), conductive hearing loss, and facial nerve palsy are indicative of posterior fossa fracture.
Battle’s Sign
(see Basilar Skull Fracture, p. 8)
Biot’s Respirations
(see Respiratory Patterns in Part 3, p. 203)
Bispectral Index Monitoring
(see also Ramsey Scale, p. 49; Riker Sedation-Agitation Scale, p. 50)
A processed EEG parameter used to measure the hypnotic effects of anesthetic and sedative agents on the brain. A sensor is placed on the patient’s forehead, and the BIS monitor translates information from the EEG into a single number (i.e., 100 = wide awake; 0 = absence of brain activity). Use of the BIS monitor does not replace the use of the peripheral nerve stimulator. Riker’s sedation-agitation scale is frequently used in conjunction with BIS monitoring to document the patient’s level of sedation.
Electrode Placement
After wiping the forehead with alcohol and drying with gauze, position the electrodes. In most cases, either side can be used, but if the patient has had a stroke, place it on the unaffected side.
Place electrode #1 at the center of forehead, about 1½ inches above the bridge of nose.
Place electrode #4 directly above and adjacent to the eyebrow.
Place electrode #3 on the temple, between the outer canthus of the eye and hairline.
Electrode #2 will then be in proper position to be secured.
Monitoring
After connecting cable, each electrode needs to self-test and “pass” before monitoring can begin. Watch the signal quality index (SQI) bar for EEG activity.
Assessment
| BIS Reading | Clinical State | EEG |
|---|---|---|
| 0 | Unresponsive | Flat |
| 1–40 | Deep hypnotic state <20, only possibility of intact protective reflexes and limited respiratory drive <40, protective reflexes possibly intact, may respond to deep stimulation | <20, approaching burst suppression <40, increased proportion of suppressed EEG |
| 41–60 | Moderate hypnotic state Deep sedation; low probability of consciousness; unresponsive to verbal stimuli, low risk of recall | Normalized low-frequency activity (determined by proprietary method) |
| 61–90 | Light hypnotic state Responds to loud verbal and deep tactile stimuli (< responsiveness with index near 60) | 60–70, beta augmentation 70–80, synchronized high-frequency activity (beta augmentation) |
| 91–100 | Awake | Normal EEG |
Troubleshooting
Replace sensors every 24 hours.
When disconnecting sensor, press release button on interference cable.
Increased EEG activity may artificially increase BIS score; be sure to check SQI.
False BIS highs may also be due to:
High-frequency power contained in pacemakers, ECG signals, warming blankets, or oscillating ventilators;
Muscle shivering, tightening, or patient motion;
Neuromuscular blocking agents that may be wearing off;
REM sleep;
Pain.
BIS lows may be due to:
Neuromuscular blockade
 Figure. Bispectral index monitoring electrode placement. (Courtesy of Aspect Medical Systems, Inc., Newton, MA.) |
Blood-Brain Barrier
(see also Anatomy: Cranial Layers, p. 5; Choroid Plexus, p. 16)
Blood-brain barrier refers to the special permeability of brain capillaries and choroid plexus that limits transfer of certain substances into extracellular fluid of CSF of brain. H2O, CO2, O2, and glucose cross easily. It is important because the blood-brain barrier is often damaged or infected when tissue is injured; damage leads to increased permeability.
Brain Attack
(see Stroke, p. 57)
Brain Death Criteria*
(see also Organ Donation in Part 11, p. 387)
Brain death diagnosis is made in the absence of hypothermia (temperature <32.2°C) and central nervous system depressants. Patient must be:
Areflexic except for simple spinal cord reflexes; pupillary, extraocular, corneal, gag, and cough reflexes are absent.
Without spontaneous respiration as determined by apnea test. To do an apnea test: Preoxygenate patient. Disconnect ventilator, and give O2 at 8 to 12 L/min by tracheal
cannula. Observe patient for spontaneous respirations. After 10 minutes, draw blood for arterial blood gases (ABGs). PCO2 must be >60 mm Hg for an accurate test. Reconnect the ventilator. Patient is considered apneic if PCO2 is >60 mm Hg and there is no respiratory movement. If hypotension and/or arrhythmia develops, reconnect ventilator. Consider other confirmatory tests.
Considered to have an irreversible condition. Duration of observation depends on clinical judgment: 12 hours is recommended when an irreversible condition is well established and no test is confirmatory; 24 hours is recommended for anoxic brain damage and no test is confirmatory.
Positive for flat electroencephalogram (EEG) (if performed).
Positive for absence of blood flow by cerebral radionuclide scan or arteriogram (if performed).
Brain Stem
(see also Cranial Nerve Exam, p. 80)
Brain stem collectively includes midbrain, pons, and medulla. It is an area that controls basic functions dealing largely with involuntary activities: blood pressure, heart rate, and respiration. Brain stem is “bottommost” in skull. Brain stem “trouble” can be identified by means of cranial nerve tests (see Cranial Nerve Exam).
Brain Structures and Function
(see Anatomy: Brain Structures and Function, p. 2)
Brain Tumors
(see Tumors, Neurogenic, p. 61)
Breathing Patterns
(see Respiratory Patterns in Part 3, p. 203)
Brown-Séquard Syndrome
Syndrome is due to incomplete lesion to one side of spinal cord, related to penetrating trauma. Assess for vibration sense, proprioception, and light touch.
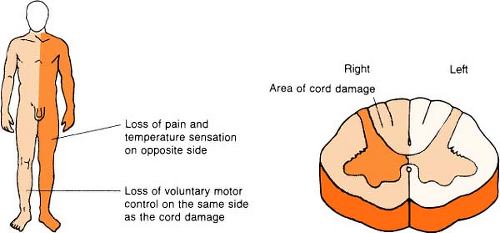 Figure. Brown-Séquard syndrome. |
Remember:
Whichever side the lesion is on (right or left), the lesion causes that side to lose motor function. The opposite side loses pain and temperature sensation.
Brudzinski’s Sign
(see also Kernig’s Sign, p. 42)
In response to passive flexion of neck, hip and knees will flex. This is due to irritating exudate around roots in lumbar region. It is a sign indicative of meningitis or for bleeding into the subarachnoid space.
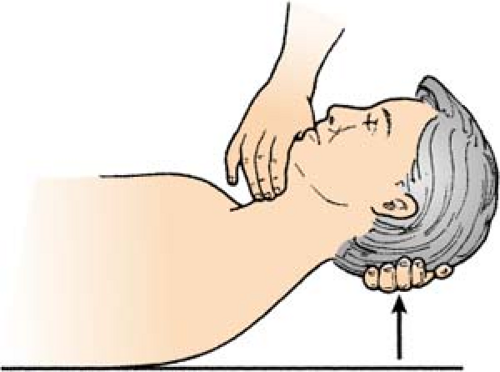 Figure. Brudzinski’s sign. (From Hickey, J. V. [2009]. Neurological and neurosurgical nursing [6th ed.]. Philadelphia: Lippincott Williams & Wilkins.) |
Caloric Test
(see also Doll’s Eyes, p. 23)
Designed to evaluate the eighth cranial nerve and the oculovestibular reflex in an awake patient, and the integrity of the brain stem on a comatose patient. It is considered to be one component in the evaluation of brain death, but is contraindicated in patients with cervical injury or a ruptured tympanic membrane. The patient is supine with the head of the bed up 30°. Instill 5 to 10 mL of water tympanically. Normal response depends on whether iced water or warm water is used, and whether patient is awake or unconscious.
A normal iced caloric test result on an awake patient (indicating eighth cranial nerve and oculovestibular reflex intact) is an initial conjugate movement of the eyes toward the side being irrigated. After about 30 seconds, the lateral gaze changes to a rapid nystagmus, pulling the eyes back to midline.
A normal iced caloric test result on an unconscious patient is conjugate, tonic eye movement toward the irrigated ear (indicating brain stem is intact). In effect, the brain has the capacity to say, “Hey, what’s that?” and tells the eyes to check it out. This is considered a good sign. It is normal in a lethargic or unconscious patient for the response to the nystagmic component (that follows the lateral movement) to be diminished or absent, since this portion is controlled by the cerebral cortex.
An abnormal iced caloric test result in an unconscious patient is associated with a poor prognosis. There may be absent or dysconjugate eye movement to the side being irrigated (indicating loss of brain stem control), and absent nystagmus.
A normal warm water caloric test result on an awake patient, while seldom used in the ICU setting, is opposite that of cold calorics. The instillation of warm water will result in conjugate eye deviation away from the side being irrigated, followed by a rapid nystagmus toward the irrigated ear.
Remember:
The mnemonic COWS (cold opposite, warm same). It refers to the water temperature used and the nystagmic portion of the reflex.
It is also possible to irrigate both ears at once. Cold irrigation will produce a slow downward deviation of the eyes, whereas warm irrigation will result in a slow upward deviation.
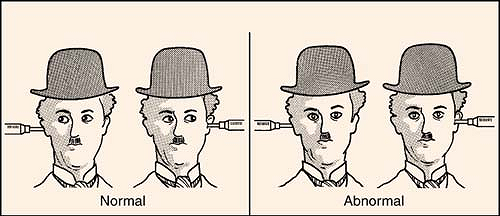 Figure. Cold caloric test on unconscious patient. (From Marino, P. L. [2007]. The ICU book [3rd ed.]. Philadelphia: Lippincott Williams & Wilkins.) |
Central Herniation
(see Herniation, p. 32)
Central Neurogenic Hyperventilation
(see Respiratory Patterns in Part 3, p. 203)
Cerebral Palsy
Cerebral palsy is a disease resulting from brain damage in a newborn, and the exact cause is difficult to determine. At highest risk are the premature or babies who have a congenital malformation. Diagnosis usually involves a period of waiting (frequently up to 18 months) for the definite and permanent appearance of specific motor problems, that is, spasticity (inability of a muscle to relax) or athetosis (inability to control the movement of a muscle). Damage is fixed and rarely shows progression or regression. While there is no specific cure or standard therapy, drugs are often used for seizure and spasm control, and braces are used for muscle imbalance. Life expectancy varies with the severity of the disease.
Cerebral Perfusion Pressure
(see also Increased Intracranial Pressure p. 35; Intracranial Pressure Monitoring, p. 37)
Cerebral perfusion pressure (CPP) refers to the pressure difference across the brain between incoming mean arterial pressure (MAP) and the opposing intracranial pressure (ICP) (see table).
Cerebral Perfusion Pressure
| CPP = MAP Minus ICP* | |
|---|---|
| Average | 80–100 mm Hg |
| Minimum for perfusion | 50 mm Hg |
| Brain death | <30 mm Hg |
| * If ICP is negative, consider it zero when calculating CPP. | |
Cerebral Salt Wasting
(see also Syndrome of Inappropriate Antidiuretic Hormone in Part 6, p. 273)
Cerebral salt wasting (CSW) is a syndrome of hyponatremia, natriuresis (excessive excretion of sodium in the urine), and a decrease in extracellular volume. Its existence as a diagnosis, and in some cases as a unique phenomenon, is greatly debated. While it closely resembles syndrome of inappropriate antidiuretic hormone (SIADH), there is one major differentiating factor. In SIADH, hyponatremia is a result of dilution. In CSW, hyponatremia is the result of primary sodium loss. However, a diagnosis of CSW can be made only if there is not excessive ADH in the body.
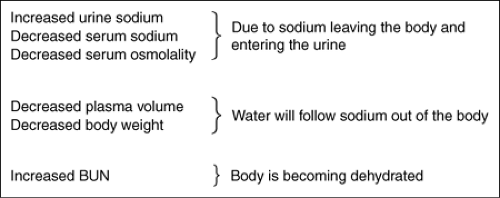 Figure. CSW findings. |
How exactly a neurologic insult leads to CSW is not yet clearly understood. It is thought that atrial natriuretic factors (ANF), substances released from the atria, play a part. ANF is also thought to cause diuresis, vasodilation, and suppression of the renin-aldosterone system.
CSW needs to be differentiated from SIADH because the treatments are the exact opposite of one another. In SIADH, the low sodium is treated with fluid restriction (to alleviate the dilutional state). In CSW, the treatment is to administer fluids (oral and hypertonic [3%] or isotonic IVs). This will replace the sodium that has already been excreted. The repletion should not be done faster than 0.7 mEq/L/hr for a maximum total daily change not to exceed 20 mEq/L. Fludrocortisone, a mineralocorticoid drug, is an adjunct to sodium and fluid replacement for CSW. It enhances sodium reabsorption in the renal tubules, allowing the body to retain more sodium.
Cerebrospinal Fluid
(see also Anatomy: Cranial Layers, p. 5; Halo Sign, p. 31; Lumbar Puncture, p. 42; Spinal Cord, p. 53)
CSF is made in lateral ventricles by choroid plexus. It is constantly produced and constantly absorbed. It circulates from ventricles in brain, around subarachnoid space and spinal cord. It is absorbed through villi into dura mater. Approximately 400 to 500 mL of CSF is made daily, or about 20 mL/hr. About 15 to 25 mL is located in each ventricle. It is characteristically clear and colorless (xanthochromic CSF is a sign of bleeding in area), with pressure of 80 to 180 mm H2O while patient is side lying.
Abnormal lab values for CSF (the following are “rules of thumb” only):
Red blood cells (RBCs). Finding RBCs in the CSF indicates hemorrhage somewhere in the central nervous system, e.g., from torn or ruptured blood vessels from injury or ruptured aneurysm. This can also be due to a bloody spinal tap.
Increased cells. Increased cells may indicate infection somewhere in the central nervous system. For example, polymorphonuclear leukocytes and increased lymphocytes may occur with viral infections and tuberculosis. If extremely large numbers of cells are present, the CSF may appear cloudy.
Lowered blood sugar. This often results from bacterial infections of the central nervous system or from SAH. A normal glucose value for CSF is 60% of serum glucose.
Lowered chloride level. Drop in chloride often results from bacterial infections of the central nervous system.
Increased protein level. Rise in protein usually occurs in the presence of a brain tumor or degenerative disease.
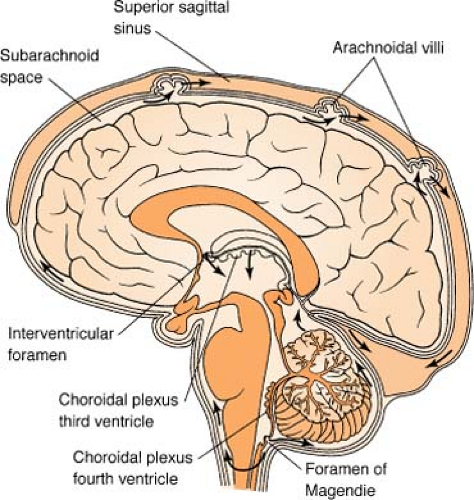 Figure. Flow of cerebrospinal fluid from the time of its formation from blood in the choroid plexuses, until its return to the blood in the superior sagittal sinus. |
Cheyne-Stokes Respiration
(see Respiratory Patterns in Part 3, p. 203)
Chiari Malformations
These are a group of abnormalities of the craniocervical junction characterized by the hindbrain descending down through the foramen magnum. The malformation is divided into three types (see figure on the next page).
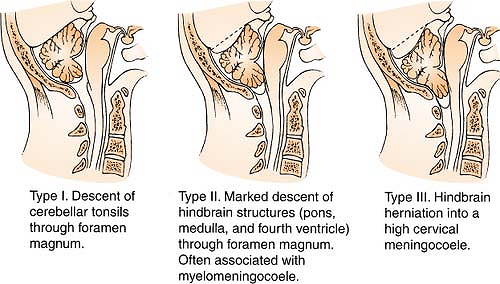 Figure. Chiari malformation. (Reprinted with permission from Palmer, J. [1996]. Manual of neurosurgery. New York: Churchill Livingstone.) |
The abnormality is rare, affecting only 1 in 10,000 to 15,000, with males more commonly affected than females. Average age for diagnosis is estimated at 30 to 40 years for adults and 11 years for children. There is a wide variance in how these patients present clinically, probably accounting for frequent delays in diagnosis. Treatment generally requires surgical intervention consisting of either (1) local decompression or (2) diversion. Local decompression consists of removing the base of the back of the skull and the posterior portions of the uppermost vertebrae. This will widen the opening of the foramen magnum. Once the bone has been removed, the membrane (dura) overlying the cerebellum and spinal cord is opened. A tissue graft is then “spliced” into the dura to provide even more room for the easy passage of CSF. Less often, diversion is used, by draining the cavity within the spinal cord with a diverting shunt tube. This can be directed from the spinal cord cavity to either the chest or the abdominal wall.
Chordoma
(see Tumors, Neurogenic, p. 61)
Choroid Plexus
The choroid plexus is a special capillary bed located in the brain that filters blood and is responsible for the production of cerebral spinal fluid.
Chvostek’s Sign
(see also Trousseau’s Sign, p. 61)
Chvostek’s sign is a twitch of facial muscles, upper lip, and eye following a sharp tap to facial nerve (seventh cranial nerve) anterior to the ear, just below the temple. It is related to a decreased serum calcium level.
Circle of Willis
The circle of Willis is an anatomic juncture representing an anastomosis of four major vessels: posterior cerebral, anterior cerebral, internal carotid, and posterior/
anterior communicating. The “circle” is the most common site for an intracranial aneurysm.
anterior communicating. The “circle” is the most common site for an intracranial aneurysm.
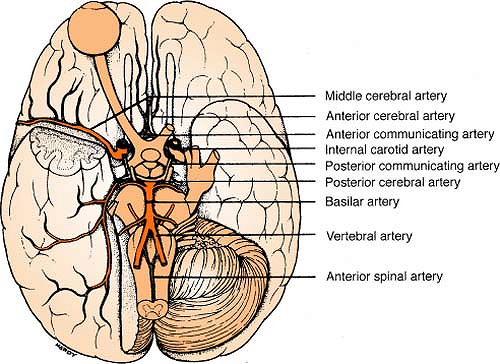 Figure. The circle of Willis seen from below the brain. |
Anterior circulation includes:
2 internal carotids (ICA)
1 anterior communicating (Acomm, AcoA)
2 anterior cerebrals (ACA)
2 posterior communicating (Pcomm, PcoA)
2 middle cerebrals (MCA)
2 ophthalmics (OA)
2 anterior choroidals
Posterior circulation includes:
2 vertebrals (verts)
2 posterior cerebrals (PCA)
1 basilar (BA)
2 superior cerebellars (SCA)
2 posterior inferior cerebellars (PICA)
2 anterior inferior cerebellars (AICA)
Many pontines
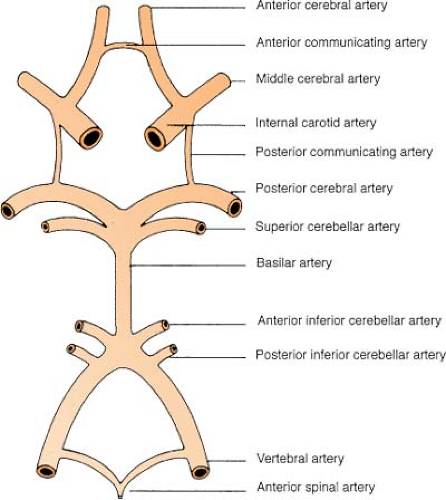 Figure. The circle of Willis. |
Cluster Breathing
(see Respiratory Patterns in Part 3, p. 203)
Coiling
(see Embolization, p. 26)
Coma
(see also Caloric Test, p. 12)
Coma is a state defined as being unconscious, unarousable, and unresponsive to touch or sound. Coma is caused by one of two things:
Damage to both cerebral hemispheres
Damage to ascending reticular activating system in brain stem
The caloric test differentiates between the two (see Caloric Test).
Consensual Reflex
A normal reflex, the consensual reflex is demonstrated by constriction of opposite pupil when light stimulates one eye.
Remember:
Consensus = both agree.
Corneal Reflex
The corneal reflex tests the fifth cranial nerve, the trigeminal. Touch cornea with wisp of cotton or place a drop of artificial tears in eyes and observe for blink reflex, or apply pressure
to supraorbital ridge and observe for facial grimacing (reflex is decreased or absent on same side as hemiplegia).
to supraorbital ridge and observe for facial grimacing (reflex is decreased or absent on same side as hemiplegia).
Cranial Nerves
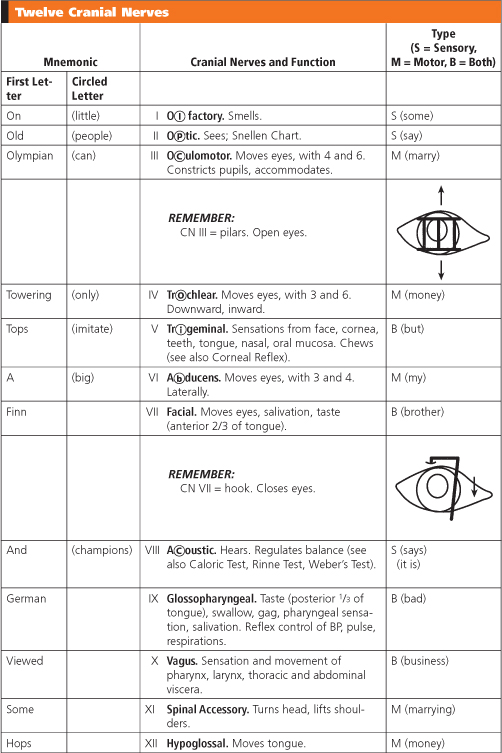
The 12 pairs of symmetrically arranged cranial nerves are attached to the brain and exit through a foramen at its base. The site where the fibers composing the nerve enter or leave the brain surface is usually termed the superficial origin of the nerve; the more deeply placed group of cells from which the fibers arise or around which they terminate is called the nucleus of origin.
To remember the names of the 12 nerves, remember the mnemonic “On old Olympian towering tops, a Finn and German viewed some hops.” But because the names of so many of the nerves begin with the same letter, also remember the mnemonic “Little people can only imitate big champions.” This gives the second letter (or third, if both second letters are the same) of the nerve. To remember the type of nerve, remember the mnemonic “Some say marry money, but my brother says (it is) bad business marrying money” (s = sensory; m = motor; b = both sensory and motor).
Twelve Cranial Nerves
 |
Cranial Nerve Exam
Cranial Nerve Assessment
| Cranial Nerve | Assessment | Comments |
|---|---|---|
| I Olfactory | Sense of smell Usually deferred | Deficits noted in only a few cases, usually with lesion in the parasellar area or a basilar skull fracture (anterior fossa) |
| II Optic | Vision Monitor while working with patient; observe for difficulty with ADLs Ask patient to identify how many fingers are being held up or to read menu or newspaper Use Rosenbaum Pocket Vision Screener to assess vision in each eye Monitor for visual field cuts by checking upper and lower quadrants while patient focuses on your nose | Common deficits, often related to a basilar skull fracture (anterior fossa), can cause blindness in one eye, bitemporal hemianopia, or homonymous hemianopia |
| III Oculomotor | Pupil constriction; elevation of upper eyelid Assess size, shape, and direct light reaction of pupils | Changes are common with a number of progressing neurologic problems |
| III Oculomotor IV Trochlear VI Abducent | Extraocular movement Tested together in conscious, cooperative patient; ask patient to follow a pencil tip through the six cardinal eye movements | Deficits are common; inability to move the eyes in one or more directions; or strabismus |
| V Trigeminal | Sensation to face; mastication muscles Often deferred If assessed, patient must be cooperative and able to accurately report facial sensation to stimulation | Deficits found in trigeminal neuralgia and sometimes with acoustic neuroma Corneal reflex assessed in trigeminal neuralgia; can assess reflex in unconscious patient |
| VII Facial | Muscles for facial expression; efferent limb of corneal reflex In cooperative patient, ask him or her to smile, show teeth, puff cheeks, wrinkle brow; observe for symmetry of face In a comatose patient, tickle each nasal passage, one at a time, by inserting a cotton-tipped applicator; observe for facial movement | Total unilateral facial weakness, called Bell’s palsy Unilateral from below the eye and down, seen in stroke Note the difference between central and peripheral facial involvement Deficits often seen in basilar skull fracture, posterior fossa |
| VIII Acoustic | Hearing and balance Usually deferred May note deficit while working with patient in the posterior fossa | Deficits with acoustic neuroma, cerebellopontine angle tumors, Meniere’s disease, and skull fracture |
| IX Glossopharyngeal X Vagus | Palate, pharynx, vocal cords, and gag reflex; tested together because of overlap In conscious patient, have patient open mouth and say “ah,” assess gag reflex In unconscious patient, assess gag reflex | Deficits common in posterior fossa lesions Gag reflex is a brain stem reflex and has prognostic value in unconscious patient |
| XI Spinal accessory | Shrug shoulders and move head side to side Usually deferred | Deficits common in posterior fossa lesions |
| XII Hypoglossal | Movement of tongue In conscious patient, ask him or her to stick out the tongue | Deficits common in posterior fossa lesions |
Craniopharyngioma
(see Tumors, Neurogenic, p. 62)
Creutzfeldt-Jakob Disease
Creutzfeldt-Jakob disease (CJD) is a degenerative neurologic disease that is rapid and fatal, similar to “mad cow” disease (bovine spongiform encephalopathy, or BSE). Though the two are similar, no correlation of a relationship between them is evident. The onset of CJD manifests itself as confusion and then it progresses rapidly to coma and death, usually within 2 years, often within 1 year. The disorder is seen in adults with an average age of 60 years. Because it is infectious, standard precautions should be taken with invasive procedures or contaminated body fluids, especially spinal fluid or brain tissue.
Csf
(see Cerebrospinal Fluid, p. 14)
Cushing’s Reflex
(see also Cushing’s Triad, p. 22)
When CSF pressure and the pressure within the intracranial cerebral arteries start to equilibrate, the cerebral arteries become compressed and begin to collapse. This compromises cerebral blood flow. Cushing’s reflex is activated, and the arterial pressure rises to a level higher than the CSF pressure, allowing cerebral blood flow to be reestablished and ischemia to be relieved. The blood pressure is maintained at a new, higher level, and the brain is protected from further loss of adequate blood flow. Cushing’s reflex causes the symptoms of Cushing’s triad.
Cushing’s Triad
(see also Cushing’s Reflex, p. 22)
The triad refers to three signs caused by Cushing’s reflex:
Bradycardia
Hypertension (with widened pulse pressure)
Bradypnea (often irregular)
It is indicative of an advanced increase in intracranial pressure, that is, the brain’s “last gasp.” The triad and the reflex are late findings, and irreversible neurologic damage may have already occurred by the time they are recognized.
Cva
(see Stroke, p. 57)
Decerebrate
Decerebration is demonstrated by extension of involved extremities with outward pronation of the wrists and hands. Legs are stiffly extended at the knees with the feet plantar flexed. This indicates disruption of motor fibers in the midbrain and brain stem and is a more ominous sign than decortication.
Remember:
“Without cerebrum” or “extension.”
 Figure. Decerebrate posturing. |
Decorticate
Decortication is demonstrated by flexion of the upper extremities and extension and internal rotation of the lower extremities on the side of the lesion. It is seen in patients with interruption of cortical nerve fibers but intact pathways through the brain stem.
Remember:
“To the core” or “without cortex.”
 Figure. Decorticate posturing. |
Delirium Tremens
(see CIWA Score in Part 11, p. 375)
Dermatomes
(see Epidural Analgesia, p. 28)
Diabetes Insipidus
(see Diabetes Insipidus in Part 6, p. 264)
Doll’s Eyes
(see also Caloric Test, p. 12; Cranial Nerve Exam, p. 20)
Also known as the oculocephalic reflex/response, Doll’s eyes testing is used on a comatose patient to check for an intact brain stem. It should never be performed on a suspected neck injury.
With eyelids held open, briskly turn the head either horizontally side-to-side (cranial nerves III, VI) or vertically up and down (cranial nerve III only).
Reflex normal (positive doll’s eyes, brain stem intact): Eyes move in the opposite direction of the head turn and then slowly drift back to the midline as if to fixate on a stationary object.
Remember:
“It’s good to be a doll!” (A positive thing!)
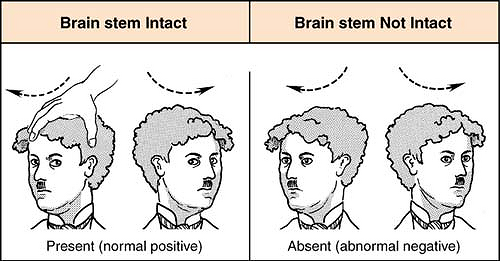 Figure. Doll’s eyes. (From Marino, P. L. [2007]. The ICU book [3rd ed.]. Philadelphia: Lippincott Williams & Wilkins.) |
Reflex abnormal (negative doll’s eyes, brain stem dysfunction from the pons to midbrain level): Eyes do not move in the sockets and instead follow the direction of head movement, remaining stationary with respect to the head.
Remember:
“Barbie is brain dead!” (Painted eyes on Barbie doll remain fixed and stare in whatever direction head is turned.)
An abnormal finding is usually followed by a cold caloric test.
Doppler Studies
(see Transcranial Doppler Studies, p. 60)
Drift
Ask the patient to close eyes and extend arms up with palms facing inward (“catch the rain” or “deliver a pizza”). Have patient count backward from 10 while maintaining elevated arms. Downward drift of one or both arms or pronation of palms indicates a positive drift and is indicative of mild hemiparesis.
Dysreflexia
Dysreflexia is a state unique to spinal cord injured patients at T5 and above, sometimes seen in patients with injury at T6 to T10. The cascade of events is triggered when an irritating stimulus (such as an overfilled bladder) is introduced to the body below the level of the injury. Since the impulse cannot reach the brain due to the injury, the body responds by initiating a reflex to increase the sympathetic portion of the autonomic nervous system. This results in spasms, narrowing of the blood vessels, and a rise in blood pressure. Nerve receptors in the heart and blood vessels detect this rise, and in an effort to control it, the brain sends a message to the heart causing the heartbeat to slow down and the blood vessels above the level of the injury to dilate. However, since the brain cannot deliver the same message to the receptors below the level of the injury, the blood pressure is unable to be regulated, and life-threatening hypertension ensues. Other common symptoms include headache, flushing, red blotches on skin above the level of the injury, and sweating above the level of the injury, due to vasodilation. Cold, clammy skin and goose bumps below the level of the injury are due to vasoconstriction. Nausea, as well as a metallic taste in the mouth, are due to vagal parasympathetic stimulation. Treatment must be initiated promptly and is aimed primarily at alleviating the precipitating stimulus, though often antihypertensives must be prescribed.
Related posts:






Full access? Get Clinical Tree


