Fig. 19.1
(a, b) CT scan. Tumor extension evaluation
Compared to CT, PET is more accurate in staging or re-staging cancer of the head and neck. After surgery and/or medical treatments, PET is used to monitor the return of cancer cells which could determine the restart of treatment. In many patients with head and neck cancers, a mass may remain after surgery, chemotherapy, and/or radiation. This mass could be visible on CT, however, it cannot determine the presence of residual cancer or if this mass was successfully treated. Consequently a PET scan could image responses from therapy and detect recurrence of treated lesions/masses.
Modern PET/CT scanners combine both imaging techniques increasing their functionality. This combination offers several gains. While the PET component illustrates the spatial circulation of biochemical activity, the CT component depicts anatomic structures. Imaging from PET is more precisely correlated with CT images in this manner. The significance of PET for the diagnosis of cervical lymph node metastases have been discussed controversially as a meta-analysis have shown that PET examination may achieve a sensitivity of up to 80 % and a specificity of 86 %, however, only half of the patients with clinical N0 neck and histologically identified metastasis could be identified by means of PET (Fig. 19.2). Nevertheless, PET/CT scanning in the post-treatment stage for assessing response and residual disease is increasingly performed and is proving to be vital in cancer treatment [1].
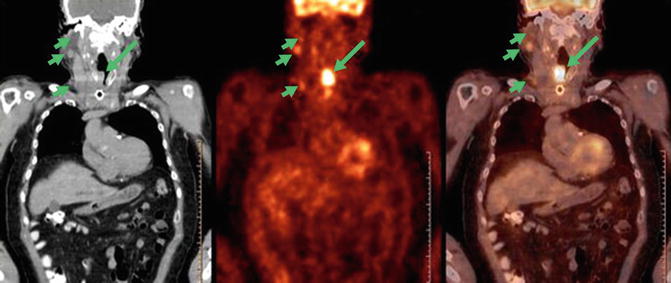
Fig. 19.2
PET CT tumor identification
Head and Neck Cancer Targeted Gene Therapy
Gene therapy in head and neck squamous cell carcinoma (HNSCC) involves delivering therapeutic genes into target tissues. Though it is still confined to trials, this evolving field is likely to progress to clinical use in combination with surgery, radiotherapy, and/or chemotherapy. HNSCC tumors serve as an ideal model for gene therapy research due to abilities of directly injecting tumors intramurally and obtaining biopsies for biomarkers evaluations.
The epidermal growth factor receptor (EGFR) is a transmembrane tyrosine kinase receptor consisting of mainly four members: ErbB1/EGFR, ErbB2/HER2, ErbB3, and ErbB4. Activation of EGFR leads to cell cycle progression that stimulates numerous antiapoptotic signals. Ninety percent of squamous cell cancers of the head and neck express high levels of EGFRs. Poor prognosis with locoregional failure and radioresistance is associated with higher levels of EGFRs via increased EGFR gene amplification.
The first gene therapy protocol for cancer was submitted in 1993. Since then, over 1,000 gene therapy and 12 HNSCC clinical protocols have been registered on Clinicals.gov. INGN 201, a promoter to encode the wild-type p53 gene, is a treatment that increases programmed cell death in tumors of HNSCC. A clinical phase III trial comparing survival to methotrexate is currently underway. Augmenting p53 in HNSCC tumors does appear to have antitumor effects. Another approach is to inhibit oncogenes as the epidermal growth factor receptor (EGFR) is greatly upregulated in 90 % of HNSCC. Inhibiting or blocking ligand binding to this receptor may prevent downstream signaling that mediate HNSCC growth. An EGFR-specific antibody, cetuximab, in combination with radiation was reported to improve survival. Although it is approved by the FDA for HNSCC, the response rate is less than 10 % as a monotherapy.
Cetuximab blocks EGFRs from the outside of cancer cells. Research has shown that cancer cells can turn proliferation and antiapoptotic signals back on by the EGFR joining with a related receptor called ErbB2, also known as HER2. Lapatinib blocks both EGFR and HER2 from the inside of cancer cells. Combining drugs that target both EGFR and HER2 may improve response in turning this signal off. An irreversible inhibitor of EGFR and HER2, the oral agent lapatinib is a recent approach in clinical studies. Current phase II studies investigate the use of lapatinib in combination with cisplatin-based chemoradiation for HPV-negative tumors. Prior to transoral surgery, lapatinib as induction therapy with carboplatin and paclitaxel is demonstrating promising results. Another such trial is assessing the progression-free survival of lapatinib and capecitabine for recurrent or metastatic disease. However, early data suggest a marginal benefit as monotherapy or in combination with platinum-based chemoradiation therapy [2].
Efficient and stable transgene expression remains a challenge in gene transfer, although several methods have been developed. Encapsulating DNA in liposomes is one such method. Genes encoding HLA-B7, interleukin (IL)-2, and E1A have demonstrated transferability by cationic liposomes. However, liposomes do not facilitate DNA integration into the genome, requiring retreatment. Conversely, viral vectors allow permanent gene integration into genomic DNA, particularly retroviruses and adenoviruses. Though transfection of DNA into tumor tissue has low efficiency, preclinical studies using naked DNA have shown moderate effects in HNSCC xenograft tumors. These injections are known to be technically challenging and usually performed by a surgeon. Ultrasound-guided injections of DNA are advantageous in identifying and avoiding blood vessels and necrotic regions.
MHC-I expression has been reported to reject leukemic cells after their gene transfer and reverse oncogenesis of transformed cells. Allovectin-7 is a plasmid DNA that expresses MHC class I molecules required for HLA-B7. In an initial phase I and phase II studies, gradual reduction in tumor size was demonstrated. Although oncolytic viruses itself do not modulate gene expression, they serve as gene delivery vectors. COX-2, which is responsible for prostaglandin production, is undetectable in normal tissue but is overexpressed in HNSCC. A COX-2 promoter-driven replication-selective adenoviral vector, Ad-COX2-E1a, demonstrated antitumor effects against COX-2-expressing HNSCC in vitro and in vivo. The most widely tested oncolytic virus in HNSCC is ONYX-015. In a phase II trial, tumor regression was observed with some demonstrating stable disease. ONYX-015 mouthwash was evaluated in the treatment of premalignant dysplasia. Histologic resolution of dysplasia was reported, however, the responses were transient. Further studies with larger sample sizes are needed to determine the effectiveness of ONYX-015 mouthwash in the treatment of premalignant oral dysplasia. A modified version of ONYX-015, called H101 was approved by the Chinese State Food and Drug Administration for cancer treatment.
A meta-analysis published in 2005 has demonstrated an increased prevalence of HPV in oropharyngeal compared to oral or laryngeal carcinoma, with HPV16 accounting for the majority of oncogenic infections. However, this systematic review only included studies on PCR-based analysis that were not combined with p16 immunohistochemistry to identify integrated HPV. HPV positive and negative tumors are reported to have different clinical and molecular presentations. HPV-positive oropharyngeal cancer patients are younger with less consumption of alcohol and tobacco. They are also inclined to have more sexual partners. The primary tumor is frequently smaller. HPV positive tumors are characterized by the inactivation of the p53 tumor suppressor gene by the oncoprotein E6, and overexpression of the p16 cell cycle protein due to the loss of negative feedback caused by the oncoprotein E7 on the retinoblastoma suppressor gene.
Studies have shown that patients with HPV positive, p16 positive, or p53 wild type tumors have better overall survival and disease free survival rates than patients with HPV negative, p16 negative, and p53 altered SCCHN. Exome sequencing revealed more mutations in HPV negative tumors. Furthermore, TP53 mutations are generally not identified in HPV positive tumors but were found in 78 % of HPV negative tumors. Therapeutic vaccines and immunotherapy targeting HPV specific epitopes are investigated in cervical cancer patients where tumor regressions are observed. Currently, a phase I trial in SCCHN is ongoing which investigates a HPV DNA vaccine using electroporation devices associated to an immunomodulatory agent, cyclophosphamide, in HPV-16 SCCHN [3].
Preclinical studies have reported enhanced antitumor effects when combining gene therapy with radiation or chemotherapy. Docetaxel in combination with EGFR antisense gene therapy resulted in reduction of HNSCC xenograft growth in vivo. Another such study resulted in significant antitumor efficacy when partial resection of HNSCC xenograft tumors was followed by a human IL-2 plasmid formulation. In radiotherapy, toxicity to adjacent structures has posed significant problems. To increase the radiosensitivity of HNSCC tumors, adenoviral particles encoding the Nijmegen breakage syndrome (NBS1) protein were used to transduce HNSCC cells. Expression of this protein resulted in enhanced sensitivity of HNSCC xenograft tumors to ionizing radiation. Combing all three modalities of transducing HNSCC xenografts to encode a tissue inhibitor of matrix metalloproteinase-2 (TIMP-2), cisplatin treatment, and radiotherapy have showed an additive antitumor effect compared to any single agent alone. Further research will improve efficacies of gene delivery and discover other potential molecular targets in HNSCC.
Related posts:







Full access? Get Clinical Tree


