Neck and Airway Injury
Paolo Campisi MSc, MD, FRCSC, FAAP
EPIDEMIOLOGY
Data on the epidemiology of pediatric neck and airway trauma are limited.
In a series of 257 pediatric head and neck trauma patients admitted to an American level I pediatric trauma center1:
Male/female ratio 2.5:1.
Median age 9.3 years.
Leading major head and neck injuries were facial and skull base fractures (32.4%) and blunt and penetrating neck and laryngeal injuries (6.7%).
Motor vehicle trauma was the leading cause of injury in children older than 3 years, and falls the most common cause in children under 3 years.
Major non-head and neck trauma was present in 35% of patients.
In a review of penetrating neck injuries in 31 children2:
This form of injury was more prevalent in males; median age was 9.5.
Motor vehicle trauma was the leading cause of penetrating injury (32%) followed by gunshot injury (23%).
Most (84%) of the penetrating neck injuries occurred in zone II of the neck (see “Classification” later in the chapter).
The mortality rate was 9%.
PATHOPHYSIOLOGY
Younger children have a relatively prominent cranium and shorter neck.
Renders them more prone to intracranial and neurologic injury following head and neck trauma.
Laryngeal injuries are also less frequent in the pediatric population due to:
A more cephalic position of the larynx that is protected by the mandible.
Elasticity of the pediatric laryngotracheal cartilaginous framework.
A narrow cricothyroid membrane that is protective against laryngotracheal separation.
Neck and airway injuries may result from blunt or penetrating trauma.
Blunt trauma causes both crush and shearing injuries:
Neck hyperextension results in crush injuries as the larynx is pressed between the offending object and the vertebral column.
Sudden changes in momentum also create shearing forces that may cause endolaryngeal mucosal tears, hematomas, and cartilage subluxations.
“Clothesline” injury: An extreme form of blunt trauma that can result in laryngeal fracture, cricotracheal separation, vascular injury, and death.
Examples of blunt trauma in children include motor vehicle accidents, bicycle accidents, sports-related injuries, blows from fists or feet, and falling or tripping on furniture or stair edges.
Penetrating trauma injury is often limited to the pathway of the penetrating object.
Degree of injury is directly related to the object’s velocity and mass.
Examples of penetrating trauma in children include motor vehicle crashes, gunshot wounds, animal bites, and falls onto sharp objects.
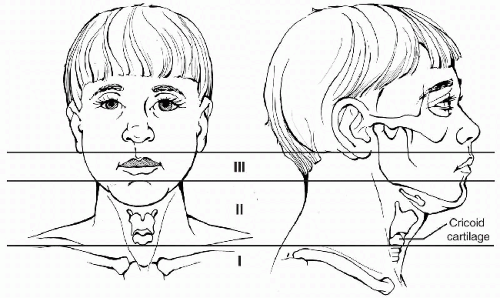 FIGURE 8-1 • Horizontal entry zones for penetrating injuries to the neck. |
CLASSIFICATION
Neck trauma can be broadly classified into blunt trauma and penetrating trauma.
Penetrating neck injuries are further classified in terms of their location in one of three anatomic zones (Fig. 8-1):
Zone I: The area between the clavicles and the inferior border of the cricoid cartilage.
Zone II: The area between the inferior border of the cricoid cartilage and the angle of the mandible.
Zone III: The area between the angle of the mandible and the skull base.
Zone I and III injuries have a higher mortality rate because surgical exposure is more difficult to achieve.
INITIAL MANAGEMENT
Evaluate according to Advanced Trauma Life Support protocol.
Promptly initiate a directed primary survey of airway, breathing, and circulation.
Assume that every neck trauma patient has both an airway and cervical spine injury until proven otherwise.
Establishing a secure airway in a child with neck trauma presents several challenges:
Potential concomitant cervical spine injury.
An attempt at intubation may further compromise an unstable airway.
Any form of surgical airway under local anesthesia may not be well tolerated by the conscious pediatric patient.
Urgent involvement of anesthesia and otolaryngology services is recommended to establish a surgical airway.
See Chapter 3 on Airway Management and Chapter 21 on Procedures for further details.Related posts:

Full access? Get Clinical Tree








