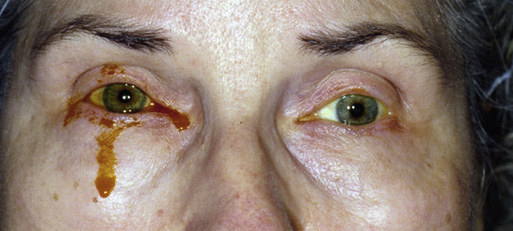
Audrey C. Ko, James T. Banta The nasolacrimal duct, commonly known as the tear duct, is a tubular structure that drains excess tears from the eyes into the nose. A complete or partial obstruction at any point along this structure is called a nasolacrimal duct obstruction (NLDO).1 There are two types of acquired NLDO: primary and secondary. Primary acquired NLDO is the most common clinical syndrome of acquired NLDO in adults and is typically caused by inflammation or fibrosis without any precipitating cause.2 Secondary acquired NLDO is caused by myriad precipitating factors, including infection, inflammation, neoplasm, and trauma. Patients affected by NLDO have disruption of normal tear drainage, causing problems that range from the annoyance of constant tearing to the more serious dacryocystitis, an inflammation of the lacrimal sac. The lacrimal drainage system consists of the superior and inferior canaliculus, the lacrimal sac, and the nasolacrimal duct. Tear drainage begins with contraction of the palpebral orbicularis oculi muscle, which acts to pump fluid through the lacrimal ducts into the lacrimal sac. The tears then enter the nasal cavity through an opening under the inferior meatus.3 In normal development, the nasolacrimal duct becomes patent to the inferior meatus of the nose during the first few weeks of life and before the onset of tear production. In 5% of newborns, the impatency persists beyond this period, and the parents may notice the clinical symptoms of congenital NLDO.4,5 Acquired inflammation originating at the eye, lacrimal system, nose, or sinuses can induce swelling of the lacrimal system’s mucous membranes, resulting in acquired NLDO. Congenital or acquired forms of NLDO can lead to stasis of tear flow and the development of secondary infections, dacryocystitis, and abscess formation. Obstruction that is not congenital may result from involutional stenosis, trauma, neoplasia, or anatomic obstructions (e.g., a deviated septum, polyps, or hypertrophied inferior turbinates). Adults with partial or complete obstruction of the nasolacrimal duct often have chronic tearing, ocular discharge, and eyelash crusting.1 More serious cases may also cause painful swelling below the medial canthus and a mucopurulent discharge from the punctum. The clinical history is used to differentiate an excess accumulation of tears caused by drainage obstruction from excess tear production. Epiphora, the accumulation of tears in the palpebral fissure with eventual overflow down the cheeks, denotes evidence of excess tearing caused by lacrimal outflow deficiency (Fig. 76-1); hyperlacrimation denotes an excess production of tears. A history of chronic allergies, sinusitis, previous nasal or sinus surgery, prior midfacial fractures, or radiation therapy may predispose patients to NLDO.6 Systemic inflammatory diseases such as Granulomatosis with polyangiitis, sarcoidosis, Crohn disease, and ulcerative colitis are other known associations.7–9 The ocular adnexa and surface structures should be carefully examined for signs of inflammation such as the presence of telangiectasias or erythema. Gross examination findings may include overflow of tears, mucoid or purulent discharge, conjunctival infection, and erythema over the lacrimal sac. Pressure over the lacrimal sac may produce a mucoid reflux from the punctum, indicative of lower system obstruction. Close attention should be given to the medial canthal region for focal swelling, fluctuance, erythema, or tenderness overlying the nasolacrimal sac, suggestive of dacryocystitis (Fig. 76-2). Fever and leukocytosis may also be present in acute dacryocystitis. Finally, a nasal speculum may be used to examine the nares for any mucosal swelling, tumors, or other anatomic abnormality that could narrow the distal opening of the nasolacrimal duct in the vicinity of the inferior turbinate.
Nasolacrimal Duct Obstruction and Dacryocystitis
Definition and Epidemiology
Pathophysiology
Clinical Presentation
Physical Examination
Nasolacrimal Duct Obstruction and Dacryocystitis
Chapter 76