Chapter 27 Myocardial Dysfunction, Ventricular Assist Devices, and Extracorporeal Life Support
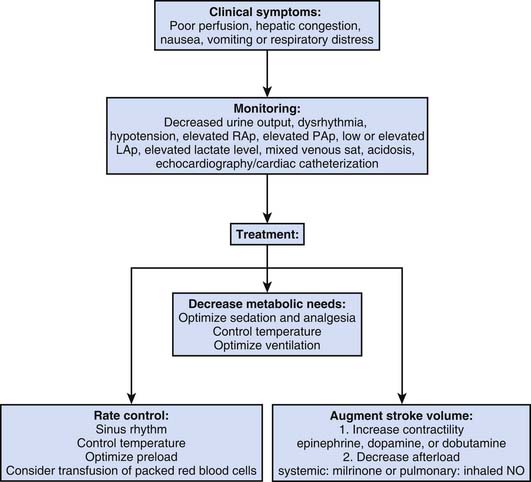
Myocardial dysfunction resulting in heart failure and low cardiac output syndrome (LCOS) is a common occurrence in the pediatric intensive care unit. The primary goal in the management of these patients is to ensure adequate tissue oxygen delivery, because an imbalance between oxygen delivery and consumption will result in further organ failure. Initial therapies to treat decompensated heart failure should target decreasing metabolic demands (i.e., work of breathing), heart rate and rhythm control, augmentation of preload, decreasing afterload, and augmenting cardiac contractility. Despite advances in medical therapy (e.g., milrinone and amiodarone),1,2 a group of patients will continue to deteriorate or require excessive vasoactive and inotropic support. This group should be evaluated for mechanical circulatory support.
Mechanical circulatory support has become an essential component of pediatric cardiac intensive care units (ICUs). Results of mechanical cardiopulmonary support in infants, children, and young adults have steadily improved in the past decade. Novel and innovative forms of mechanical circulatory support are being developed while extended indications are currently being explored. Extracorporeal life support (ECLS) remains the most commonly deployed form of mechanical support.3,4
Low Cardiac Output Syndrome
LCOS describes a clinical and biochemical state where there is inadequate systemic oxygen delivery (DO2) to meet the metabolic demands of the patient. This condition has been described since the 1960s, and multiple studies have documented the predicted change in physiologic parameters. LCOS is frequently seen in patients with severe sepsis, myocarditis, and cardiomyopathies and after pediatric cardiac surgery.5 Postoperative physiologic changes resulting from cardiopulmonary bypass, residual lesions, cardioplegia, ventriculotomy, changes in the loading conditions of the myocardium, or myocardial ischemia during aortic cross-clamping all may contribute to the development of LCOS. A variety of proinflammatory triggers are activated during cardiopulmonary bypass as a result of blood contact with foreign surfaces, ischemia, reperfusion, tissue trauma, and temperature changes. This complex inflammatory response includes complement activation, cytokine release, leukocyte and platelet activation, and the expression of adhesion molecules.6 LCOS has been reported to affect up to 25% of infants and children, typically occurs between 6 and 18 hours after cardiac surgery, and results in longer intensive care stay and increased mortality.7 It is associated with elevated systemic and pulmonary vascular resistances, impaired myocardial function, and arrhythmias. When unrecognized or inadequately treated, LCOS can result in irreversible end organ failure, cardiac arrest, and even death. Prevention, early recognition, and optimal treatment are essential components for reversing its course.
Although detailed assessment of oxygen delivery in critically ill children is extremely challenging, numerous hemodynamic and biochemical parameters can help guide the bedside clinician. Arterial lactate and mixed or central venous saturation are important biochemical markers in patients with LCOS. An elevated lactate level on admission and one that rises at 0.9 μm per hour postoperatively is associated with major adverse events including death in infants after cardiac surgery.8 Furthermore, lower mixed venous saturation may increase the predictive power of elevated arterial lactate levels for mortality after pediatric cardiac surgery.9–13 The predicted changes in cardiac output have been systematically demonstrated in newborns following the arterial switch operation for transposition of the great vessels.14 The median maximal decrease in cardiac index (32%) occurred approximately 6 to 12 hours after separation from cardiopulmonary bypass, and nearly a quarter of these newborns reached a nadir of cardiac index that was less than 2 L/min/m2. The drop in cardiac index was coupled with a rise in the calculated systemic and pulmonary vascular resistance. Perfusion strategy with either low-flow bypass or circulatory arrest was not associated with postoperative hemodynamic or other nonneurologic postoperative events.14
Decreasing Oxygen Consumption
LCOS has been an active area of research, and multiple reviews of current therapies are available to guide the intensivist.15–17 VO2 is determined by tissue metabolism and is increased during periods of increased muscular activity, infection, hyperthermia, or with increased levels of catecholamines. Supportive care for decompensated heart failure begins with strategies aimed at decreasing the child’s metabolic demands. These strategies often include basic critical care therapies such as intubation and mechanical support for respiratory insufficiency, analgesia and sedation, and treatment of anemia (Figure 27-1). Likewise, temperature control is a routine but important part of intensive care, and even a modest increase in body temperature can result in major increases in systemic VO2 during the early postoperative period.18




Pharmacologic Treatment of Pediatric Heart Failure
In contrast to adult patients, tremendous heterogeneity exists between the etiology and pathophysiology of congestive heart failure in pediatric patients. Despite these differences, treatment strategies for pediatric patients have traditionally followed the recommendations extrapolated from large, randomized, multicenter trials in adult patients because of a lack of pediatric clinical trials. Symptom management with digitalis and diuretics formed the basis of early therapy (~1970s) of pediatric patients with congestive heart failure. Angiotensin-converting enzyme inhibitors (ACEI) exert favorable effects on cardiac remodeling and survival in adults with congestive heart failure. Their role in children is less clear. A randomized, placebo-controlled trial in children evaluated the effect of ACEI in patients with a single ventricle by measuring exercise capacity, but this study failed to demonstrate a beneficial effect.19
β-Blockade utilization in pediatrics primarily has been extrapolated from the positive effects seen in adult trials that demonstrated a reduction in mortality and risk of hospitalization with the use of carvedilol.20–21 A few reports have been made of the efficacy of propranolol in children with severe congestive failure as a result of left-to-right shunts22 and of metoprolol in children with dilated cardiomyopathy.23 Single-center trials have demonstrated both improved ejection fraction with the use of carvedilol in children awaiting heart transplantation with dilated cardiomyopathy24,25 and a delayed time to transplantation or death.25 However, the most recent and largest multicenter, randomized, double-blind, placebo-controlled trial of carvedilol for children and teenagers with symptomatic systolic heart failure failed to demonstrate an improved survival benefit.26
Milrinone, a phospodiesterase-3 inhibitor, has emerged as an important “inodilating” agent that is widely used in children after open heart surgery.1–2,27–29 A landmark study showed that the prophylactic use of milrinone was associated with a decreased likelihood of LCOS in children after certain types of open-heart surgery.28 This benefit is thought to result from both improved myocardial contractility as well as pulmonary and systemic vasodilatory effects.2,28 Milrinone reduces right ventricular (RV) and left ventricular (LV) afterload through systemic and pulmonary vasodilatation and improves diastolic relaxation (lusitropy) of the myocardium through its enhanced cyclic adenosine monophosphate (cAMP)–dependent reuptake of calcium after systole.30,31 A loading dose of 25 to 50 μg/kg generally is administered followed by a continuous infusion at doses between 0.25 to 0.75 μg/kg/min.
Calcium sensitizing agents (Levosimendan) have been shown to improve cardiac function and survival in adults with decompensated heart failure.32 but pediatric data is scarce.33–37 Nitric oxide is another therapy that may improve right heart failure.38–39 Adult patients who undergo open heart surgery and receive triiodothyronine supplementation have demonstrated a dose-dependent increase in cardiac output that has been associated with an improved clinical outcome. However, a recent systematic review concluded that there is lack of evidence that triiodothyronine supplementation is beneficial in the prevention of morbidity and mortality in children undergoing cardiac surgery.40
Fenoldopam, a selective dopamine-1 receptor agonist, causes systemic vasodilatation and increased renal blood flow, with improved renal function.41–43 Its use in critically ill adult patients with renal dysfunction has become routine. Two recent meta-analyses have concluded that the use of fenoldopam in critically ill adult patients at risk of acute kidney injury appears to decrease the development of acute tubular necrosis, the requirement for renal replacement therapy, overall patient mortality, and length of ICU stay.44–45 One study also demonstrated a reduction in the time on mechanical ventilation.44 However, few data exist regarding the use of fenoldopam in neonatal or pediatric patients. One retrospective study evaluated the use of fenoldopam in neonates after cardiopulmonary bypass with poor urine output despite conventional diuretic therapy and demonstrated a significant improvement in diuresis.46 However, a subsequent prospective trial failed to demonstrate a beneficial effect.47
Terlipressin is a synthetic long-acting analogue of vasopressin with a higher affinity for vascular V1 receptors than vasopressin. Terlipressin has been used in adult patients to treat extremely low cardiac output,5 but its application in children is limited. Terlipressin demonstrated an improvement in respiratory, hemodynamic, and renal indices in postoperative pediatric cardiac patients with refractory LCOS.48–49 While these results are encouraging, further investigation with prospective randomized trials are needed to provide data regarding the efficacy and safety of terlipressin in infants and children.
Mechanical Circulatory Support
Historical Perspective
Since 1953, when John Gibbon first utilized extracorporeal perfusion in the operating room, the indications and utilization of this therapy have continued to expand. Technological advances in ECLS have afforded support for thousands of patients per year with a variety of respiratory and/or cardiac indications. As of July 2009, a total of 37,092 pediatric and neonatal patients were registered patients within the Extracorporeal Life Support Registry.50
Early trials of ECLS were marked by mixed results. In 1985, Bartlett51 reported the first successful use of ECLS in a newborn. Since then, neonates with diagnoses of meconium aspiration syndrome, persistent pulmonary hypertension, and congenital diaphragmatic hernia have been treated for severe respiratory failure that is unresponsive to conventional therapies.52,53 ECLS was first used for cardiac support in the 1970s by Baffes, but it was not until the 1990s that ECLS became a common therapeutic technique for this patient population.54–55
In 1971, DeBakey reported the first successful use of a VAD in adults.56 During the past 20 years, the favorable results seen in the adult population has prompted the adaptation of adult technology for pediatric patients. Two pulsatile paracorporeal devices were introduced for use in children, the Medos-HIA and the Berlin Heart. Worldwide experience with these devices to support the neonatal and infant population as a bridge to either recovery or transplantation is increasing.
Mechanical Support Devices
Short-Term Mechanical Support Devices
Extracorporeal Life Support
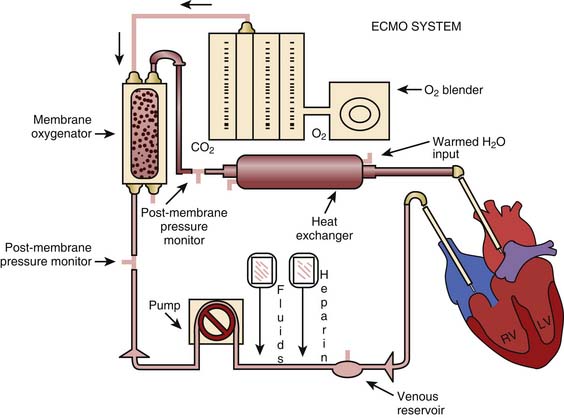
ECLS is primarily utilized for short-term support of patients with decompensated heart failure who are unresponsive to medical therapy. Adaptations to the traditional cardiopulmonary bypass circuit have resulted in the standard ECLS circuit (Figure 27-2). The ECLS cannulation is initiated by placement of vascular cannulas within the patient’s circulatory system.
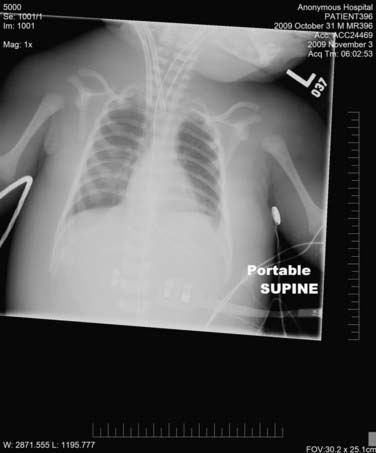
Venoarterial (V-A) ECLS provides both biventricular and typically pulmonary support. It is important to note that complete cardiac support cannot be provided by V-A ECLS because of incomplete drainage of the right heart. Routine cannulation for V-A ECLS occurs via one of three arterial and venous access points: (1) The transcervical approach places the venous cannula in the right atrium via the right internal jugular vein and the arterial cannula in the ascending aorta via the right carotid artery; (2) the transthoracic approach with direct cannulation of the right atrium and aorta through a median sternotomy is utilized for postoperative cardiac patients who either cannot be weaned from cardiopulmonary bypass or require mechanical circulatory assistance in the immediate post-operative period; and (3) femoral artery and vein cannulation is an option for older/larger children via the femoral artery and vein. The transcervical and transthoracic approaches are the preferred methods for small children. Figure 27-3 demonstrates a chest radiograph evaluation of cannula placement in a patient supported by V-A ECLS.
Venovenous (V-V) ECLS provides pulmonary support without cardiac support. In V-V ECLS a single cannula is placed in the right atrium through a transcervical approach. This cannula provides both inflow and outflow for the circuit. V-V ECLS can improve RV dysfunction as a result of oxygenated, pH-balanced blood flowing to the lungs, thus decreasing pulmonary vascular resistance and right heart afterload. In addition, improved filling of the LV can occur through decreasing RV overdistension. Likewise, the absence of an aortic cannula prevents the increase in LV afterload seen with venoarterial ECLS. However, at times the indirect cardiac effects of V-V ECLS do not adequately improve ventricular dysfunction and conversion from V-V ECLS to V-A ECLS is required. See Table 27-1 for a comparison of V-A versus V-V ECLS.
Table 27–1 Venoarterial vs. Venovenous ECMO
| Venovenous ECMO | Venoarterial ECMO | |
|---|---|---|
| Organ support | Pulmonary | Pulmonary and cardiac |
| Cannulation site | Transcervical or femoral | Transcervical, transthoracic, or femoral |
| Pump | Roller or centrifugal | Roller or centrifugal |
| Length of support | Days to weeks | Days to weeks |
ECMO, Extracorporeal membrane oxygenation.
The no membrane oxygenator VAD is an adaptive technique to traditional ECLS that several centers have utilized. This form of ECLS eliminates the oxygenator from the standard circuit configuration. This technique allows for mechanical circulatory support while limiting both the harmful inflammatory effects of the oxygenator and reducing the initial need for anticoagulation.57 It allows the ECLS device to be utilized as either an RV assist device, LV assist device, or a biventricular assist device.
Extracorporeal Life Support Physiology
Patient circulatory physiology is altered by the initiation of mechanical circulatory support, and it is important to understand how ECLS affects these patients. Mechanical circulatory support affords recovery of myocardial function through a variety of mechanisms. Alteration of both RV and LV preload and afterload occurs to varying degrees based on which device is utilized and how it is utilized. Some of these alterations can be deleterious. Adequate decompression of the left heart decreases left atrial hypertension and reduces cardiac wall stress, cardiac work, and myocardial oxygen consumption, allowing for improved coronary perfusion. Mechanical circulatory support of the LV allows for reverse molecular remodeling with normalization of heart failure and apoptosis markers, normalized expression of genes involved in calcium homeostasis, cell growth, and differentiation, and up-regulation of structural proteins.58 With adequate venous drainage, both right atrial and left atrial pressures are lowered. This effect is important to prevent complications such as pulmonary edema or hemorrhage, pleural effusions, ascites, superior vena cava syndrome, or stroke. Likewise, a low to normal central venous pressure is important for patients who have experienced cardiac arrest and are at risk for ongoing cerebral ischemia as a result of cerebral edema and increased intracranial pressure.
Extracorporeal Life Support Indications and Contraindications
It is widely accepted that all patients considered for mechanical circulatory support should have either a reversible physiologic process or be a candidate for a bridge to transplant or a bridge to destination therapy. The time frame in which recovery is expected and the severity of cardiac and/or other organ failure is used to guide medical personnel regarding optimal selection of a mechanical circulatory support device. Appropriate patient selection and stabilization is vital to maximize survival and outcome with any mechanical circulatory support system. The ELSO Registry Outcomes as of July 2009 are listed in Table 27-2.
Table 27–2 ELSO Registry Outcomes as of July 2009
| Category | Total | % Survival |
|---|---|---|
| Neonate | ||
| Respiratory | 23,191 | 75 |
| Cardiac | 3749 | 39 |
| ECPR | 492 | 37 |
| Pediatric | ||
| Respiratory | 4188 | 56 |
| Cardiac | 4564 | 46 |
| ECPR | 908 | 38 |
ECPR, Extracorporeal cardiopulmonary resuscitation; ELSO, Extracorporeal Life Support Organization.
From Extracorporeal Life Support Organization, Ann Arbor, Mich.
Myocarditis
The clinical course of patients with myocarditis is variable. Some patients present with subclinical disease, others have an indolent course that progresses to dilated cardiomyopathy, and a subset of patients demonstrate fulminant disease. Those with fulminant acute myocarditis often experience a rapidly progressive course leading to death. Without mechanical circulatory support, patients with a fulminant course had expected survival rates of only 25% to 50%.59–61 With the aggressive utilization of ECLS as a bridge to transplantation or recovery (or VAD if a longer recovery time is anticipated), survival rates for patients with any form of myocarditis are now reported to be as high as 90% to 93%.62–64 It has been suggested that the institution of ECLS may aid in the normalization of ventricular geometry, a phenomenon that is referred to as reversible remodeling. This process is thought to improve ventricular dysfunction because of favorable influences on the neurohormonal cardiovascular milieu and unloading of the LV.65 For patients with the most severe disease, that is, end-stage dilated cardiomyopathy resulting from fulminant myocarditis, the use of mechanical circulatory support without transplantation has resulted in survival rates as high as 67% to 80%.66–68
Postcardiopulmonary Bypass
Failure to wean from cardiopulmonary bypass occurs in approximately 1% to 3.2% of pediatric congenital cardiac surgery cases.69–71 Individual institutions have reported survival rates to hospital discharge between 32% and 54% for pediatric patients who require ECLS after cardiac surgery.70–77 One small series has reported a survival rate as high as 80%.69 However, the July 2009 ELSO registry report for postoperative cardiac surgery patients younger than 16 years reported an overall survival rate of only 40%.50 All of these patients demonstrate LCOS refractory to medical management as detailed in prior sections. It has been demonstrated that in patients with decompensated heart failure, a rising blood lactate level >0.75 mmol/L/hour on serial measurements despite escalating inotropic support may accurately predict a poor outcome.10 For this patient population, it is anticipated that cardiac arrest or end-organ dysfunction will occur. The use of mechanical circulatory support is a widely accepted tool to support the vital organs while allowing for myocardial recovery.78–80 It is imperative that this group of postoperative cardiac patients be evaluated for residual cardiac defects before considering mechanical circulatory support. Diagnostic or interventional cardiac catheterization may guide treatment pathways or be therapeutic. On occasion a patient’s condition may warrant immediate mechanical support in order to safely proceed with cardiac catheterization. In these instances it is feasible to obtain hemodynamic and angiographic data or to perform therapeutic interventions in the cardiac catheterization laboratory. Balloon valvuloplasty or angioplasty of aortic arch obstructions, device closure of residual atrial or ventricular septal defects, coiling of aortopulmonary collateral vessels, and/or balloon or blade atrial septostomy all may be crucial interventions to improve cardiac output and allow for separation from mechanical circulatory support. If these defects cannot be managed in the catheterization laboratory, prompt return to the operating suite will be required. Residual cardiac defects, if left untreated, have been shown to be nearly universally fatal for patients requiring mechanical circulatory support.80
The use of ECLS for postcardiotomy support in neonates and infants with single-ventricle physiology remains controversial and continues to be considered a relative contraindication in some centers. The 2009 ELSO report lists a 34% survival rate for ECLS use in patients following the stage I Norwood procedure,50 which is lower than for other postcardiotomy patients.50,81
Extracorporeal Cardiopulmonary Resuscitation
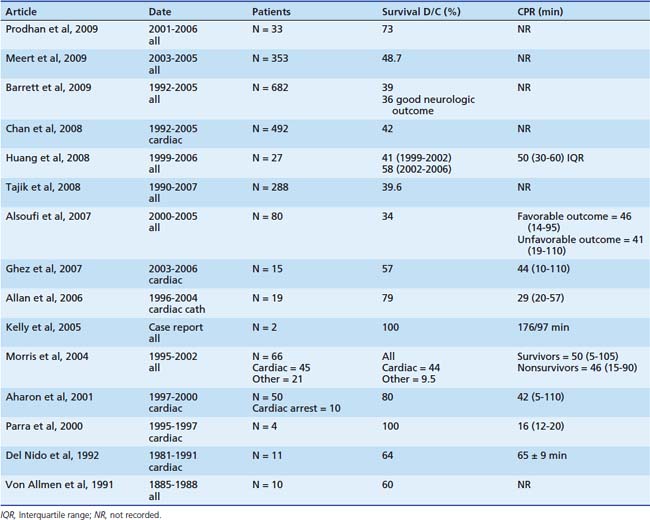
In-hospital cardiac arrest in children continues to be associated with dismal outcomes despite advances in cardiopulmonary resuscitation (CPR). A prospective multicenter observational study from the National Registry of Cardiopulmonary Resuscitation reported a good neurologic outcome for 73% of survivors of an in-hospital cardiac arrest, yet the rate of survival to hospital discharge was only 27%.82 Another multicenter observational study from the Pediatric Emergency Care Applied Research Network reviewed in-hospital cardiac arrests that occurred during an 18-month period between 2003 and 2004. It also reported a good neurologic outcome for 76% for survivors and an improved (49%) rate of survival to hospital discharge with the utilization of extracorporeal CPR. Both reviews excluded out-of-hospital, do-not-resuscitate, or neonatal ICU patients.83 However, while neurocognitive outcome has improved for survivors of cardiac arrest, the duration of CPR has been inversely proportional to survival. One center demonstrated that a witnessed in-hospital cardiac arrest of >30-minute duration was universally fatal without the utilization of ECLS.84 This knowledge has led to an emerging interest in the use of ECLS for patients who have failed to reestablish a perfusing rhythm and adequate circulation with conventional CPR rescue techniques. The American Heart Association guidelines for in-hospital pediatric cardiac arrest now recommend consideration of ECLS during CPR if the conditions leading to the arrest are likely to be reversible or amenable to heart transplantation.85 However, wide variability in patient selection and the ability to institute ECLS in a timely fashion (5 to 176 minutes) has led to variable success reports ranging from 0% to 100%.86–95 Table 27-3 presents a summary of the current literature on ECPR. Thus large centers have increasingly dedicated resources for the rapid deployment of ECLS, utilizing a team that is immediately available to cannulate with a pre-primed circuit. The 2009 ELSO Registry for neonatal and pediatric patients supported with ECLS following cardiac arrest reported a survival to hospital discharge rate of 38%.50
Myocardial Failure: Bridge to Transplantation
While heart transplantation is the treatment of choice for patients with end-stage myocardial failure, many children die every year waiting for a suitable organ to become available. As a result, mechanical circulatory support is now increasingly utilized as a bridge to heart transplantation. The most common indications for ECLS as a bridge to transplant include end-stage congenital heart disease, cardiomyopathy, and graft rejection after heart transplantation. To date, no randomized controlled trials have been performed in the pediatric age group to determine if mechanical circulatory support as a bridge to cardiac transplantation confers improved survival for patients with myocarditis. Children with myocardial failure resulting from myocarditis demonstrate increased short-term survival when treated with ECLS and transplantation,67 however; long-term survival reports suggest that bridge to transplantation may only be indicated for patients with giant cell or the acute form of myocarditis but not those with the fulminant form.62–6396
Factors that dictate which mechanical circulatory support device is used include patient size, the need for pulmonary support, and duration of wait time. Complications associated with ECLS generally limit the duration of support with this device to approximately 2 weeks, although support that lasts >4 weeks has been rarely reported. As long as complications precluding transplant have not developed, there should be no arbitrary cutoff for duration of support. A recent review of the United Network for Organ Sharing Database from 1995 to 2005 evaluated both clinical status at transplantation and risk factors for short- and long-term mortality of patients supported with various mechanical circulatory support devices. This study revealed that 30-day survival was significantly decreased for patients who received a bridge to transplant with ECLS versus VAD; long-term (10-year) survival was not affected. Not surprisingly, preoperative severity of illness also predicted early survival following cardiac transplantation. The overall 10-year survival rate was 56.8%.97
ECLS has been the mainstay of therapy for small children and neonates in the United States for short-term support (~2 weeks) because of a paucity of devices for this age group. The use of paracorporeal pulsatile assist devices (Berlin Heart and Medos HIA) for neonates in European countries has demonstrated early promising results.98–100 The utilization of this technology is in its nascent stage in the United States. However, a retrospective review that compared survival outcomes of children supported with ECLS versus Berlin Heart to heart transplantation or recovery at Arkansas Children’s Hospital favored the use of the Berlin Heart (57% vs. 86%).101
Malignant Dysrhythmias
Mechanical circulatory support is an essential therapy for patients with malignant dysrhythmia that is unresponsive to pharmacotherapy. A subset of patients with acute fulminant myocarditis presents with refractory LCOS and dysrhythmia that further compromises end-organ perfusion. If these patients do not rapidly respond to antiarrhythmic agents, many progress to cardiac arrest and death. In this scenario, mechanical circulatory support may be beneficial as a bridge to recovery or transplantation.63 Several potentially lethal tachyarrhythmias, such as supraventricular tachycardia, junctional ectopic tachycardia, or ventricular tachycardia, can occur congenitally or are acquired in the postoperative period as a result of the ingestion of toxic substances or medications.102–104 Again, ECLS can allow time for resolution of dysrhythmia, for medical treatment to take effect, and/or for recovery of cardiac function.
Refractory Respiratory Failure
Severe neonatal respiratory failure refractory to maximal medical therapy that requires ECLS is the most common indication for ECLS. Diagnoses include meconium aspiration syndrome, congenital diaphragmatic hernia, persistent pulmonary hypertension of the newborn, sepsis, respiratory distress syndrome, or other congenital lung abnormalities. Three randomized controlled trials involving neonates have been conducted and all reported that ECLS improved the survival rate.53,105–107 It has been reported that of infants treated with ECLS, the proportion of infants with congenital diaphragmatic hernia has been increasing, whereas the proportion with respiratory distress syndrome, meconium aspiration syndrome, and sepsis has been decreasing.108 However, the overall patient survival for this group remains at 75%.1 A recent report, the first to perform a systematic comparison of neonatal ECLS practice patterns and respiratory failure deaths between countries, demonstrated distinct differences between the United States and the United Kingdom. It concluded that U.S. clinicians seem more willing to utilize ECLS for persistent pulmonary hypertension of the newborn and congenital diaphragmatic hernia. This difference in practice pattern was correlated with a decrease in the U.S. neonatal death rate from congenital diaphragmatic hernia in comparison with the United Kingdom.109
During the past 2 decades, successful treatment of pediatric patients with ECLS is increasingly being described in patient groups that would have been excluded in the past. ECLS is now considered for patients with trauma, immunosuppression, underlying bleeding disorders, sickle cell disease, status asthmaticus, pulmonary embolism, established multiple organ system failure, and more. However, reported survival rates are variable. For example, whereas a survival rate of 94% is reported in patients treated with ECLS for refractory status asthmaticus,110 that of immunocompromised patient populations is only 31% to 36%.111–112 Even of greater concern is that although case reports of survival with good neurologic outcome exist for the hematopoietic stem cell transplant population, review of the ELSO database demonstrates an almost universal fatal outcome for these patients.113–114 The duration of ECLS required until successful decannulation is often longer for respiratory indications of use. This finding is likely due to the fact that parenchymal lung disease often requires a longer period of recovery than does myocardial dysfunction. The most common diagnosis in the pediatric respiratory ECLS group of patients is acute respiratory distress syndrome. Overall survival for this group of patients remains at 56%.50 Although no randomized controlled trials for pediatric patients with refractory respiratory failure have been performed, a prospective, observational study with matched control subjects demonstrated improved survival of ECLS patients when compared with conventional support.115
Contraindications
If a patient has been selected as an appropriate candidate for consideration of mechanical circulatory support, then few absolute contraindications exist. While each institution may have slight variations of this list of contraindications, it is generally accepted that weight <2 kg, irreversible cardiac failure without the option for transplantation, severe neurologic dysfunction, severe intracranial or intraabdominal bleeding, and lethal congenital abnormalities are all absolute contraindications. Technical limitations would include an inability to obtain vascular access as a result of thrombosis, abnormal anatomy, or prior surgery. As previously discussed, when considering a postoperative cardiac patient for mechanical circulatory support, it is prudent to rule out the possibility of a residual cardiac defect. Furthermore, cardiac arrest is not an absolute contraindication if rapid resuscitation is available and the underlying etiology is deemed to be reversible.
Critical Care Management During Extracorporeal Life Support
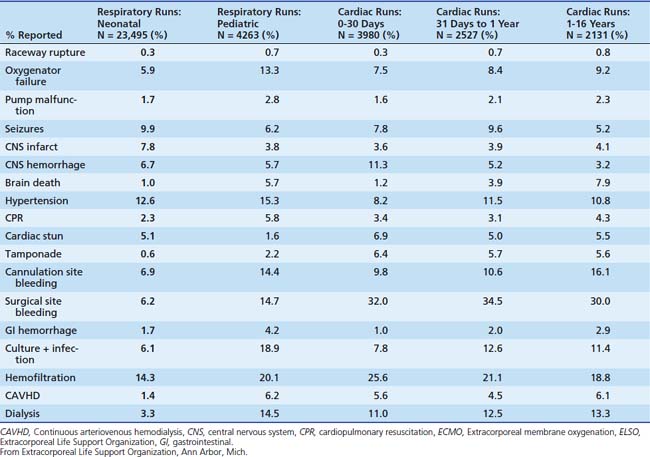
Patients who require mechanical circulatory support are critically ill, often with loss of multiple end-organ function. It is not surprising that complications occur with a greater frequency for this group of patients than for other critically ill pediatric patients. The basic management principles are discussed in this section. Table 27-4 will be referred to frequently throughout this section because it summarizes the most common reported complications for pediatric patients supported by ECLS as of July 2009.
Cardiac Output
When assessing the hemodynamic state of a patient, one must consider to what degree the patient is contributing to cardiac and or pulmonary circulation versus the ECLS device. The amount of flow provided by the ECLS device is easily obtained from circuit monitors, although least accurately from revolutions per minute (rpm)/circuit diameter calculations. For most cardiac ECLS patients, flow is initiated at 120 to 150 mL/kg/min. However, it is important to note that flow should be adjusted to fit the physiologic needs of each patient. Patients with single-ventricle physiology or sepsis may require higher flows approaching 200 mL/kg/min to support their metabolic needs. Assessment of the patient’s intrinsic cardiac output is often unobtainable. However, indirect evaluation of the patient’s cardiac output is possible through assessment of arterial systolic blood pressure, pulse pressure, heart rate, organ perfusion, mixed venous oxygen saturation, and lactic acid levels on a given flow rate. Comparisons of these variables over time allow the clinician to make decisions regarding the adequacy of circulatory support or the readiness to wean from support. An echocardiogram also can provide valuable information and help guide therapy. Mixed venous saturation is measured in the venous return portion of the circuit, with a goal of 65% to 80% in acyanotic patients. However, if a “left-to-right” shunt exists, such as a left atrial vent, the mixed venous saturation will be falsely elevated. In cyanotic patients an arterial venous oxygen saturation difference (Sa-VO2) of 20% to 25% is typically targeted. Serial lactate measurements often are a helpful aid in the assessment of total end-organ perfusion. A delay in clearance may occur in patients with ongoing hepatic dysfunction, sepsis, low CO, and end-organ hypoperfusion. An approximation of the relative contributions of the patient and circuit pulmonary parameters is possible. This assessment is permitted through analysis of serial patient and circuit blood gas assays such as pH, PCO2, and PaO2, with consideration of the mechanical ventilation settings (includes fraction of inspired oxygen [FIO2] and PEEP), circuit flow rate, CO2 sweep rate, and circuit oxygen concentration.






Full access? Get Clinical Tree


