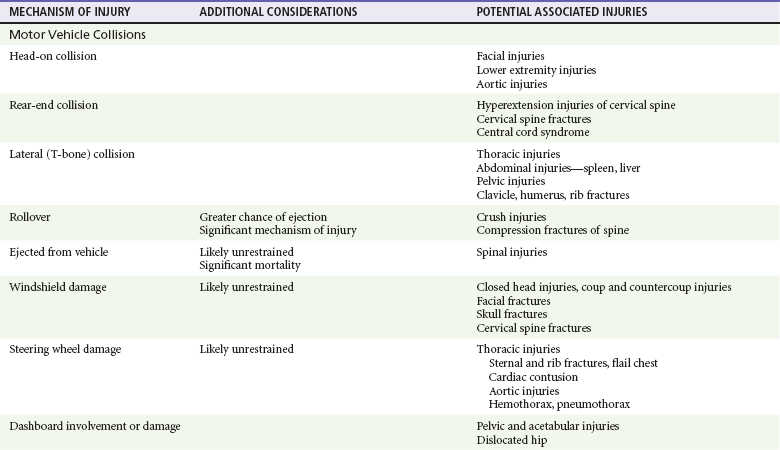
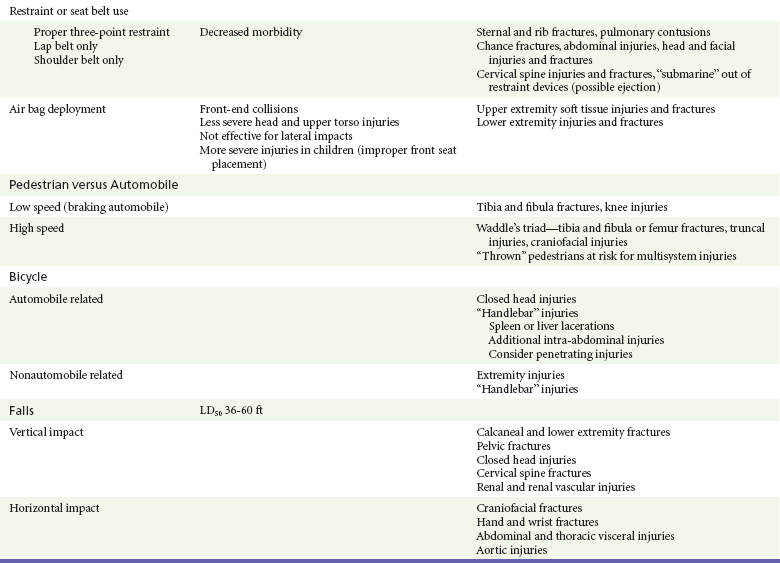
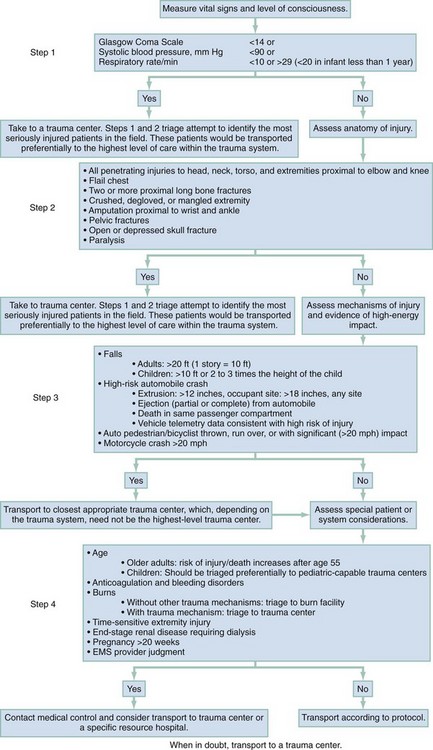
Chapter 36 The care of the injured patient remains one of the mainstays of emergency medicine practice. Emergency physicians play a vital role in the stabilization and diagnostic phases of trauma care. Management of trauma patients involves complex, time-dependent decision-making, leadership capability, and technical skill. Proper resuscitation can enhance functional outcomes, even in severely injured patients.1 In 2009, there were 117,176 deaths from unintentional injury, of which 31% were motor vehicle related. Accidents continue to be the leading cause of death in people aged 1 to 44 years.2 The motor vehicle fatality rate has declined over the past decade from 15.3 deaths per 100,000 population in 1999 to 11.0 deaths per 100,000 in 2009.3 Likewise, the number of people injured in motor vehicle collisions (MVCs) has declined as well, to 2.2 million people in 2009.4 Firearm deaths continue to be of significant concern in the United States. In 2009, there were 31,228 deaths by firearm.2 The economic cost of traumatic injuries is staggering. It is estimated that the total cost of injuries that occurred in 2000 is $406 billion; this includes medical costs and lost productivity. Motor vehicle and fall injuries account for 22% ($89 billion) and 20% ($81 billion) of this total, respectively.5 Many of these injuries are avoidable. Proper use of lap and shoulder belts can reduce the risk of fatal injury from an MVC; it is estimated that in 2009 alone, seatbelts saved 12,713 lives.6 In 2009, 29% of occupant MVC fatalities involved individuals who were not restrained.3 The number of MVC fatalities has been decreasing steadily since 1994, but there is room for improvement. Young adults continue to use restraints at a lower rate than the national average, but usage by this age group is increasing. Eighty-four percent of adults aged 25 to 69 years use seatbelts compared with 81% of 16- to 24-year-olds.7 It is interesting to note that there are racial differences in seat belt use. Seventy-nine percent of blacks use seatbelts compared with 84% of whites and 89% of other races.7 It is estimated that proper restraint use in vehicles by occupants age 5 years and older would have prevented 3688 MVC-related deaths.6 Child safety seats reduce the risk of death in passenger cars by 71% for infants and by 54% for toddlers ages 1 to 4 years.8 Educational and law enforcement initiatives addressing seat belts, proper child restraint, drinking and driving, gun safety, and fall prevention can assist in raising public awareness. For example, the National Highway Traffic Safety Administration (NHTSA) “Click It or Ticket” campaign increased belt use in 41 of 50 states and the District of Columbia during a 2-month time period.9 NHTSA recently finished a small pilot study of a device to provide haptic feedback to the gas pedal when drivers attempted to drive over 25 mph. The researchers noted 100% seat belt use when this technology was implemented.10 Further study of new technologies may improve restraint use. The effect of firearm laws on decreasing firearm violence is less concrete (even though a decrease in injuries related to firearm violence has been seen).11 Further study is needed to determine the impact of legislation, public education, and prevention programs on firearm violence. The first document to set criteria for categorizing hospitals as trauma centers was promulgated by the American College of Surgeons (ACS) Committee on Trauma in 1976.12 As other groups recognized the importance of structured trauma care, legislation and funding to promote the development of trauma systems grew. In the early 1990s the Health Resources and Services Administration developed the Model Trauma Care System Plan, a well-designed framework for progress measurement in trauma systems. Unfortunately, this program lost funding in 2006. As of 1998, 38 states and the District of Columbia had at least one critical element in place for a formal trauma system.10 More up-to-date data are not readily available because the program was the main source for this information. Data on the benefit of regionalized trauma systems are convincing. The National Study on the Costs and Outcomes of Trauma showed a 25% reduction in mortality for severely injured patients who received care at a level I trauma center versus patients at a non–trauma center.13 A meta-analysis of 14 studies demonstrated an overall 15% decline in mortality caused in the presence of a trauma system.14 However, this apparent reduction in fatalities may be confounded by other factors. A nationwide study suggests that mortality reduction could not be solely attributed to the presence of a trauma system because its impact was small and statistically not significant. Rather, the presence of a primary seat belt law and mean per capita income were associated with a reduction in occupant mortality rates, whereas rural population and speed limits faster than 65 mph were associated with an increase in mortality rates.15 As new trauma systems mature, more research will be needed to guide implementation of new system strategies to further reduce morbidity and mortality from traumatic injury. One goal of the out-of-hospital trauma system is to transport the patient to the closest appropriate facility in a timely manner. Problems with over-triage and under-triage occur. Most efforts are aimed at reducing under-triage (transport of severely injured patients to lower-level trauma centers), which may result in preventable morbidity and mortality owing to a delay in definitive care. Over-triage (transport of minimally injured patients to higher-level trauma centers) has no deleterious effects on patient care; however, it may contribute to unnecessary resource utilization and potential overcrowding in tertiary care, level 1 trauma centers. The Centers for Disease Control and Prevention (CDC) worked with experts in 2006 to establish the Field Triage Decision Scheme. Based on initial work by the ACS Committee on Trauma, this scheme outlines triage criteria to assist in proper triage of the injured patient (Fig. 36-1).16 The scheme is endorsed by the American College of Emergency Physicians, the ACS, and many other organizations. Limitations to effective use of regionalized trauma systems remain. Hospital crowding, ambulance diversion, lack of specialist on-call availability, and reimbursement issues all contribute. In addition, from 1990 to 2009 the number of hospital emergency departments (EDs) in nonrural areas declined from 2446 to 1779. During this time, 1041 EDs closed and 374 hospitals opened EDs.17 Trends such as this increase the burden of emergency care on those remaining hospitals, potentially compromising care. Future funding and legislative decisions at the state and national levels will have a significant impact on the future of high-quality trauma care in the United States. The emergency physician faces significant clinical uncertainty when a multiple trauma patient arrives in the ED. Much of the diagnostic dilemma and subsequent evaluation can be guided by knowledge of the mechanism of injury. Although mechanisms of injury alone are not good predictors of major trauma,18 common patterns of injuries can be anticipated and specifically assessed in ED patients. Table 36-1 outlines several blunt trauma mechanisms of injury with potential associated clinical findings. Table 36-1 Blunt Trauma Mechanisms and Associated Injuries LD50, the height of fall that would be fatal for 50% of those falling. Injury patterns can differ significantly between adults and children subjected to similar mechanisms of trauma. The major anatomic distinctions relate to the smaller size and surface area, larger head-to-body ratio, and less protected abdominal cavity of the child. As a result, children are more vulnerable to multisystem injury in blunt trauma, more frequently sustain significant head and intra-abdominal injuries, and are more at risk for hypothermia.15–18 Accidents were the fifth leading cause of death in 2009.2 Elder patients commonly sustain extremity, craniofacial, and closed head injuries. The majority of these occur as the result of a fall or an MVC. Elder trauma patients typically have normal, age-related changes in organ system function related to decreased cardiopulmonary functional reserve, decreased renal function, decreased bone density, and cerebral atrophy. These changes can increase susceptibility to shear forces and other aspects of trauma.19 Comorbidities and preexisting medication use further complicate the management of elder trauma patients. Lower extremity weakness, gait disturbances, decreased visual acuity, and the use of psychotropics, antihypertensives, and sedatives have been associated with falls in elders, resulting in major injury.20 The use of these medications, particularly antihypertensives, should not be considered causative in trauma patients with hypotension until acute hemorrhage has been assessed and managed. In addition, anticoagulants, antiplatelet drugs, and aspirin are commonly prescribed, and their effects should be suspected and reversed if possible in elder trauma patients. The majority of life-threatening injuries that require intervention by out-of-hospital providers are related to airway, breathing, and circulation (the ABCs). Preventing aspiration of gastric contents and providing adequate tissue oxygenation are the primary goals of endotracheal intubation. Although controversy exists regarding the use of out-of-hospital rapid sequence induction,21–27 securing an unprotected airway is essential in this phase of trauma management. Tension pneumothorax is the fundamental threat to adequate ventilation and requires immediate needle thoracostomy. Systemic hypotension with impaired end-organ perfusion necessitates treatment in the trauma patient, despite the debate surrounding controlled hypotension versus aggressive fluid resuscitation. In the United States, rapid transport to the nearest appropriate facility is one of the fundamental concepts in trauma management. Much of the controversy regarding various out-of-hospital approaches to the ABCs is rooted in attempts to limit transport times and avoid further infringement on the “golden hour” of trauma care. In contrast, physician-operated emergency medical services (EMS) systems more aggressively manage airway and ventilatory issues and are more likely to commit out-of-hospital time resources to establishing hemodynamic stability before transport.28,29 Rural EMS systems in the United States, where transport times may be prolonged because of the distance to a receiving facility, may benefit from more advanced interventions, such as rapid sequence induction and intubation and more aggressive fluid resuscitative measures. For level 1 trauma centers, the ACS requires the presence of a surgeon or an appropriate representative (e.g., a fourth- or fifth-year surgery resident) to be present in the hospital 24 hours a day. The attending surgeon is expected to be present in the ED no later than 15 minutes after the ED arrival of trauma patients (Box 36-1).30 As the specialty of emergency medicine has evolved and the number of residency-trained and board-certified emergency physicians has increased, the need for a surgeon for all trauma patients has been increasingly debated; study has shown equivalent outcomes when the trauma team is led by either a surgeon or an emergency medicine physician.31–33 Optimal patient care is best provided in a collaborative, patient-centered manner. The priorities in the treatment of trauma patients are similar to those for any other life-threatening condition. Securing the airway, maintaining ventilation, controlling hemorrhage, and treating shock are first priorities because of their crucial importance for survival. The emergency physician should give consideration to the worst possible injury and act accordingly until the diagnosis has been confirmed or excluded. The consequences of an overzealous evaluation are more acceptable than those of a missed injury. Based on ATLS, the phases of ED care are divided into the primary survey with interventions and adjuncts, consideration of transfer, the secondary survey and adjuncts, and continued monitoring and disposition.34 Airway and Breathing.: Proper assessment and management of airway, oxygenation, and ventilation in the trauma patient are of utmost importance but can be challenging. In a review of 44,404 trauma patient admissions and 2594 deaths, airway management was responsible for 16% of preventable errors likely contributing to trauma mortality.35 The goals of airway management are threefold: airway protection, adequate oxygenation, and adequate ventilation. Airway protection is necessary in many trauma patients. Airway obstruction necessitates immediate intervention. Obstruction from debris, blood, or vomitus may be easily removed with suction. Neck or facial trauma may cause more complicated problems. Swelling, distorted anatomy, and hematoma formation may all contribute to impending obstruction. Early airway control is safest because these conditions may rapidly worsen. Inability to adequately protect the airway, such as in patients with depressed levels of consciousness, is another indication for intervention. Airway control is recommended in patients with significant head injury (Glasgow Coma Scale [GCS] score below 9).36 Low GCS scores from intoxication, and not injury, may not necessitate intubation, as loss of airway reflexes cannot be predicted by GCS alone in this group.37 As a general rule, all trauma patients should be placed on supplemental oxygen. Adequate oxygenation has a direct effect on outcome of many trauma patients. In head-injured patients, hypoxia and extreme hyperoxia in both out-of-hospital and hospital phases of resuscitation have been associated with poorer outcomes.38–41 Hypoxia may also worsen outcome in spinal cord injury.42 Maintenance of arterial oxygen concentration (PaO2) above 60 mm Hg has been recommended.43 Inadequate ventilation, which may lead to respiratory acidosis, can be noted by the rate and quality of respirations. Signs of inadequate oxygenation may be more subtle and include agitation and restlessness. Assessment for injury that may compromise oxygenation, ventilation, or both requires careful inspection and auscultation of the chest. Signs of such compromising injury include increased work of breathing, tachypnea, penetrating wounds, flail segments, tracheal deviation, and distended neck veins. In determining the need for more aggressive airway management, these data are put into the context of the patient’s overall presentation. Certain ventilatory problems, such as pneumothorax or hemothorax, may require tube thoracostomy in addition to intubation. Early intervention is preferable in the tenuous patient. Once the decision to intubate the patient has been made, many considerations are taken into account. If the patient’s condition allows, a brief neurologic examination before paralytics can be helpful in determining the extent of injury. Also, cervical spine injury precautions should be considered for patients with blunt trauma and gunshot wounds to the neck. Rapid sequence induction and orotracheal intubation with in-line cervical stabilization provide a safe method. There have been no reported cases of spinal cord injury from orotracheal intubation if proper stabilization has been applied.44 There are many approaches to airway control, and many alternative devices, such as video-assisted laryngoscopy, the flexible fiberoptic scope, and the intubating laryngeal mask airway, are now available to assist in intubation. In particular, video-assisted laryngoscopy causes less cervical spine motion and results in improved vocal cord view when compared with direct laryngoscopy.45,46 However, the choice will be based on clinical scenario and physician comfort. Nasotracheal intubation is generally undesirable in trauma patients owing to the lower success rate36 and higher complication rate47 than that for orotracheal intubation, the potential for abrupt rises in intracranial pressure, and the relative contraindications of severe midface trauma or severe basilar skull fracture. Surgical airways are indicated in cases of failure of or contraindication to orotracheal or nasotracheal intubation. Cricothyrotomy is the preferred method, although it is performed in less than 0.5% of cases.48 Given the rarity of use, we recommend the use of the four-step method described by Brofeldt and colleagues, either with or without a bougie.49,50 A variety of devices for percutaneous cricothyrotomy are also available that show good success rates and are easy to use.51–53 If there is any question about the ability to identify the cricothyroid membrane, the traditional surgical approach with a vertical incision should be used. Circulation.: Assessment of hemodynamics and circulatory status is of critical importance after the airway has been evaluated and controlled and adequate ventilation has been ensured. The assessment of circulation is multidimensional. Clinical indicators of adequate perfusion include mental status, skin color and temperature, heart rate, blood pressure, and capillary refill. A normal finding for any single sign does not rule out shock. Mental status changes associated with hypoperfusion can include anxiety, agitation, or sedation. Cool, pale skin or extremities with delayed capillary refill suggest inadequate perfusion and shock. A normal heart rate, blood pressure, or both can be present despite significant hemorrhage. Conversely, tachycardia may be seen without evidence of significant volume loss. Control of external hemorrhage is crucial. Traditionally, direct pressure to external bleeding sites has been advocated, and the use of tourniquets has been discouraged. The use of direct pressure on the bleeding site remains first-line therapy; recent data have suggested the more liberal use of tourniquets for massive extremity bleeding that is not easily controlled.54–57 Similarly, recent studies of newer hemostatic agents have shown potential application in both combat and out-of-hospital settings.58–60 Intravenous access is required early in the assessment of circulation. Two large-bore (14- or 16-gauge) intravenous catheters are recommended. Routine intravenous access may be difficult or unobtainable in certain cases. Intraosseous vascular access can be obtained rapidly in both pediatric61 and adult62 patients and allows the safe infusion of large amounts of fluid or blood products. Compact, battery-operated intraosseous drills have recently been introduced. Ultrasound-guided peripheral venous access by both nurses and physicians should be considered in patients when blind peripheral attempts are unsuccessful.63,64 Central venous access may also be indicated in the appropriate clinical scenario or based on physician discretion. The use of ultrasound has been shown to increase successful vein cannulation and decrease complications in the placement of central venous lines.65–68 Central venous pressure measurements may be used to direct resuscitative efforts but should not delay definitive care. The choice of fluids for resuscitation includes crystalloid, colloid, and blood products. Fluid replacement is generally based on a 3 : 1 ratio of fluids to blood loss. There are few clinically significant differences between lactated Ringer’s and normal saline. The debate regarding the choice of fluid for resuscitation is ongoing. No indisputable advantages of colloids have been demonstrated. Therefore the less expensive and more readily available crystalloids are the routine mainstay as first line of therapy. No clear benefit to the use of hypertonic saline has been established.69–72 Current ATLS guidelines standardize the ratio of replacement fluids to loss and recommend 2 L of crystalloid be infused in all patients in shock, followed by blood products. O-positive blood should be used except in women of childbearing age. Type-specific blood should be used when available, but emergent transfusion should not be delayed. The use of the antifibrinolytic agent tranexamic acid has been shown to decrease mortality in trauma patients at risk of major bleeding.73,74 The concept of “permissive hypotension” is based on the concern that resuscitation to normal blood pressures may increase bleeding from a site that is contained and not actively hemorrhaging.75 Clinically, restoration of normal blood pressure is delayed until active bleeding foci have been ruled out. Although data exist to support this strategy,75,76 a Cochrane review of the six available clinical trials meeting inclusion criteria did not support (or disprove) the use of early or larger-volume intravenous fluids in uncontrolled bleeding.77 Permissive hypotension is contraindicated in the management of traumatic brain injury because of the risk of hypoperfusion.78,79 The extended focused abdominal sonography in trauma (eFAST) examination should be performed on all patients as an adjunct to the assessment of circulation. The presence or absence of free intra-abdominal, intrathoracic, or intrapelvic hemorrhage or pneumothorax diagnosed by ultrasound will direct the management of trauma patients. Pericardial effusions or tamponade can be readily identified. In addition, ultrasound evaluation of the inferior vena cava may be useful in the overall assessment of fluid status in resuscitation.80–85
Multiple Trauma
Perspective
Epidemiology
Trauma Systems
Principles of Disease
Management
Emergency Department
Primary Survey

Full access? Get Clinical Tree


Multiple Trauma
Only gold members can continue reading. Log In or Register to continue



