Key Clinical Questions
What are the major disease manifestations and complications of multiple sclerosis?
How are exacerbations of multiple sclerosis treated?
What are treatment options for complicating symptoms of multiple sclerosis, such as fatigue, bladder dysfunction, and spasticity?
What disease-modifying agents are available to treat multiple sclerosis? What are their major toxicities?
Introduction
Epidemiology
The peak age of onset between 20 and 40 years, and it has a twofold higher incidence in women. It has long been observed that latitude of residence in childhood is a risk factor for the development of the disease. MS is rare in equatorial areas, and the prevalence rises sharply with increasing distance from the equator. The relation of MS prevalence to latitude and altitude suggests that increased sun exposure in childhood protects against MS, but more recent work favors a genetic predisposition to MS that is geographically clustered.
Genetic factors play a major role in the development of MS, and a family history is common. The major histocompatibility complex allele HLA-DRB1*1501 and two cytokine receptor genes, the interleukin 7 receptor alpha chain gene (IL7RA) and the interleukin 2 receptor alpha chain gene (IL2RA), have been implicated. Susceptibility to MS is likely polygenic, with the contribution of most genes to MS risk being relatively small. Clusters of MS cases have suggested an infectious trigger, although the search for a specific viral or bacterial cause of MS has been thus far fruitless.
Clinical Presentation
Multiple sclerosis is characteristically a relapsing and remitting disease, but there is great variation in its course. Common presenting symptoms of MS are summarized in Table 213-1. Weakness, numbness, or both in one or more limbs are common first symptoms. Patients may have paresthesias in the extremities or a band-like tightness around the trunk or limbs. The legs may feel heavy or difficult to control. Neck flexion may cause a sensation of electric shocks in the shoulders, back, and occasionally in the thighs. This finding, known as the Lhermitte sign, may also be present in cervical spondylosis, vitamin B12 deficiency, radiation myelopathy, and other conditions affecting the cervical spine.
| Paresthesias and other sensory disturbances | 37–45% |
| Motor weakness | 20–27% |
| Disturbance of gait or balance | 13–35% |
| Vision loss or optic neuritis | 15–17% |
| Diplopia and/or vertigo | 10–13% |
Certain acute or subacute clinical syndromes are particularly characteristic of MS, although they also occur in association with other diseases of the nervous system. Optic neuritis most often presents with a deep aching sensation in the eye for a day or two, followed by rapid visual loss over several days or less. It is usually unilateral, but may be bilateral or sequential. Swelling of the optic nerve head (papillitis) is seen in 10% of patients, the majority of cases being retrobulbar and, therefore, having a normal disc head. In acute myelitis, patients develop paraparesis or paraplegia over hours to days, with extensor plantar responses, ascending paresthesias, a sensory level on the trunk, and impaired sphincter function. Cerebellar ataxia and brainstem syndromes are also frequent. Sphincter dysfunction, especially urinary urgency, is common as the disease progresses.
Common examination findings include hyperreflexia, extensor plantar responses, lower-extremity ataxia, impaired rapid alternating movements, and loss of vibration and proprioception. Evidence of optic neuropathy may be present, either obvious (visual loss) or subtle (afferent pupillary defect). Previous episodes of optic neuritis cause optic nerve atrophy. Somewhat less frequent findings include nystagmus, intention tremor, spasticity, dysarthria, and paraparesis. Unilateral internuclear ophthalmoplegia is another characteristic finding but is not common.
Natural History
At first, most patients (85%) fall into the category of relapsing-remitting MS, undergoing periodic symptomatic flares (relapses) with incomplete recovery (remission). Emotional stress and infections have tentatively been associated with flares. The postpartum period is another frequent time of relapse; MS often abates during pregnancy. In 10% of patients, the disease has little response to treatment and a progresses inexorably from the onset (primary progressive MS). A minority (5%) have “benign” MS, with few relapses and little disease progression 10 to 15 years after diagnosis. Most patients with relapsing-remitting MS eventually develop a secondary progressive course characterized by steady neurologic deterioration and pathologically, by a progression from demyelination to neuronal loss. The cervical cord is particularly prone to disease in these cases.
Diagnosis
The diagnosis of MS requires evidence of dissemination of disease in both space and time, although the time-honored requirement for the occurrence of clinical relapses has been replaced by imaging evidence of lesions of varying ages and in several central nervous system locations (Table 213-2). The major diagnostic test for MS is now magnetic resonance imaging (MRI). Typical lesions on MRI are bright on T2-weighted and fluid-attenuation inversion recovery (FLAIR) images, consistent with high water content (Figure 213-1). Early lesions are isodense on T1-weighted images and display enhancement with gadolinium, but more advanced ones may be T1 isodense, indicating necrosis (“black holes”). Typical locations include the periventricular regions, corpus callosum, cerebellar peduncles, and spinal cord.
| The diagnosis of multiple sclerosis requires demonstration of dissemination of lesions in both time and space, as follows: | |
| Dissemination in sime | Dissemination in space |
| ≥ 2 attacks | Objective clinical evidence of ≥ 2 lesions |
| OR | OR |
| Simultaneous gadolinium-enhancing and non-enhancing lesions on MRI at any time | ≥ 1 T2 lesion in at least 2 of 4 typical locations (periventricular, juxtacortical, infratentorial, spinal cord) |
| OR | |
| A new T2 and/or enhancing lesion on follow-up MRI, in addition to a previously documented MRI lesion | |
The diagnosis of primary progressive MS requires one year of insidious neurological progression, plus 2 of 3 of the following:
| |
Figure 213-1
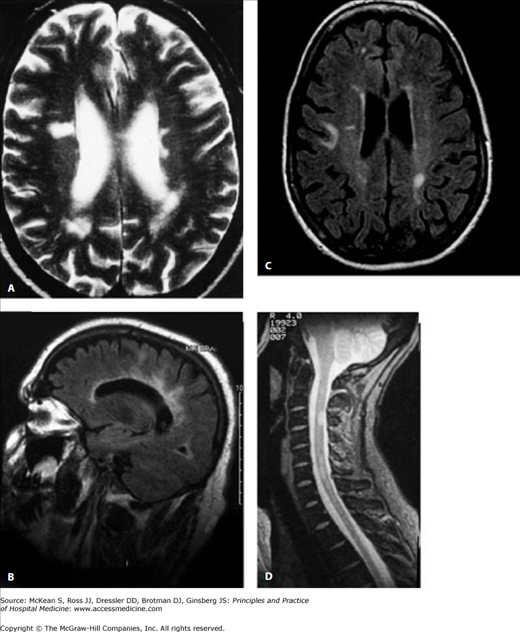
Multiple sclerosis. T2-weighted and fluid-attenuated inversion recovery (FLAIR) sequence MRIs demonstrating multiple plaques in the periventricular white matter (A), emanating radially from the corpus callosum (“Dawson fingers”; B), a “C-like”–shaped lesion in the right subcortical white matter that is created by interruption of the lesion by the adjacent cortex (C) and cervical spinal cord (D). The radial orientation and periventricular location of cerebral lesions are typical of MS. (Reproduced, with permission, from Ropper AH, Samuels MA. Adam’s & Victor’s Principles of Neurology. 9th ed. New York: McGraw-Hill, 2009. Figure 36-1.)
Lumbar puncture is helpful but not mandatory for the diagnosis of MS. The cerebrospinal fluid (CSF) may display a minimal increase in lymphocytes (< 50/mm3
Related posts:
 Strategies for Cost-Effective Care
Strategies for Cost-Effective Care
 Building, Growing, and Managing a Hospitalist Practice
Building, Growing, and Managing a Hospitalist Practice
 Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
 Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist
Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist

Full access? Get Clinical Tree


