Fig. 1.1
Maimonides eighteenth-century portrait of Maimonides, from the Thesaurus antiquitatum sacrarum by Blaisio Ugolino (Wikipedia accessed March 11th 2014)
During the Middle Ages, Catholicism became dominant in the religious world. Much of the responsibility of the care of the sick fell to monastic orders. Unlike in the Jewish tradition, monks, while learned, were not usually physicians and had not studied anatomy or completed an apprenticeship with a medical teacher. In addition, the Roman Catholic Church declared that the shedding of blood was incompatible with holding holy office (the Ecclesia Abhoret a Sanguine edict of 1163). Henceforth, monks, the educated class, were prohibited from performing surgery. But up to that point, following in the Greco-Roman tradition and the teachings of the Talmud, many operations such as wound care, lithotomy, amputations, reduction of dislocations, and even Cesarean sections had been carried out in monasteries. The barbers who had shaved the monks’ heads and who had often assisted the monks took over the practice of surgery often with disastrous results [7]. Monks were left to rely on herbal and other ancient methods of care. For example, leprosy was endemic in medieval Europe. While avoidance of contact with the sick and their isolation had been advocated both in the Bible and by Jewish law, in 1313, Philip the Fair of France ordered that all lepers should be burned [8]. Fortunately, before this edict could be fully executed, some 17,000 monasteries of Saint Lazarus (a brother of Martha and Mary who is said to have been raised from the dead by Christ, Fig. 1.2) were set aside for these victims who were then cared for, mostly in complete solitude by monks, who were themselves lepers. These facilities were known as lazarettos and numbered over 19,000 in Europe alone. By the end of the sixteenth century, the pestilence had died out in that part of the world and lazarettos were abolished by Louis XIV in 1656, the proceeds from their sale used to build hospitals [8].

Fig. 1.2
Christ Raising of Lazarus, Athens, twelfth to thirteenth Century (From Wikipedia accessed March 11th 2014)
Several other diseases were assigned to saints and adopted by specific monastic orders. The order of St. Anthony was founded in the eleventh century to take care of sufferers of acute ergot poisoning which was named St. Anthony’s fire [9]. Midwives had also used controlled amounts of ergot to induce abortions for centuries. St. Anthony’s fire was later determined to be due to tainted rye and the convulsions associated with consumption of the bread have been claimed to be the accusations of bewitchment that spurred the Salem witch trials between 1692 and 1693 (Fig. 1.3). There was said to be an abundance of rye in the region [10, 11]. The association of a saint to a disease was often determined by the manner in which the saint died. St. Appolonia had her teeth and jaw shattered and it was to her that one prayed for relief of toothache. St. Vitus’ dance (Sydenham chorea) was named after the patron saint of dance. St. Agattin who suffered a double mastectomy was the patron saint of nursing women and St. Valentine oversaw the care of epileptics. For cure of these and many other disorders, pilgrimages to the designated monasteries where they where cared for by monks who where proclaimed to have special knowledge of the respective disorders.
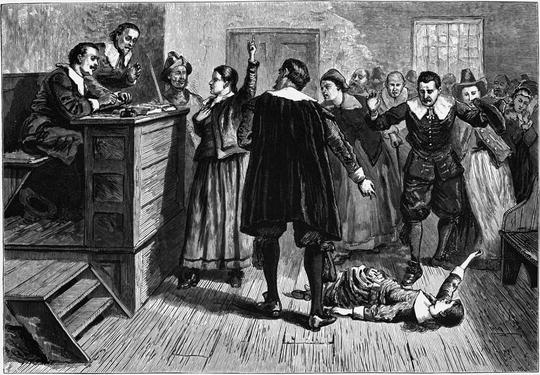
Fig. 1.3
The Salem witch trials were a series of hearings and prosecutions of people accused of witchcraft in colonial Massachusetts between February 1692 and May 1693. These trials resulted in 20 people being executed, most of them women. The central figure in this 1876 illustration of the courtroom is usually identified as Mary Walcott (from Wikipedia accessed March 11th 2014)
Eighteenth to Late Nineteenth Centuries
In its earliest stages, the missionary movement from the West mainly centered on enlightened views of healing and incorporated them into theology and practice. In essence, Western medicine was brought to a world beyond the west, often for the first time and became established as the main source of health care for the region. Common remedies and purges might be dispensed, programs for community hygiene commenced, anesthesia introduced, planning for medical facilities started, and research established into finding the cause for diseases. But while medical knowledge and new means of treatment were advanced, people on missions found out that they were exposed to and often in conflict with other concepts of the causes of illnesses. Radically different modes of treatment and contrary understanding of what constitutes human wellness were difficult notions to embrace. In addition, the economics of missions changed. Ethical and theological issues arose as to how or if treatment should be paid. Medical missions changed many assumptions as to how hospitals should function and what role women should play.
Although monasteries were declining as a center for healing, major achievements were made by many medical missionaries dispatched and funded often by religious organizations or governments in the United Kingdom and other parts of Europe. Perhaps one of the first physicians sent from a Protestant Church and sponsored by Germany and Denmark was Dr. Kaspar Gottleib Schlegemilch in 1790. Sadly he died of dysentery in India only a month after his arrival and thus was able to achieve little [12]. He was followed by other Dutch and German doctors who did not stay long or also died of tropical diseases [12]. But many more physicians and other healthcare providers travelled to distant lands, some with little medical training. Missions usually lasted for years, the health of the provider often the determining factor. During this time, clinics and facilities were established and supply lines set up. Only within the past few decades have missions been arranged for days or weeks to areas where infrastructures already exist.
The need for medical training was slowly becoming realized, but not all missionaries were so enlightened. The Rev Halvor Ronning, his wife, Hannah, and sister Thea went to China from the United States (Later they became Canadian citizens) in 1891 to found a Lutheran mission in the interior of China in the city of Fancheng in Hubei Province. Once there they established a school and had great success extending medical care to the indigent, including abandoned female newborns and breaking the boundaries of outmoded traditions by offering “modern” education to young men and especially to women. Hannah would not permit girls with bound and broken feet into the school which went on to become the largest establishment in the area. Although they had no medical training they quickly learned from the two doctors (who also had no more than 2 years instruction) and some nurses who joined them at the mission site how to dispense medicines, apply dressings, and instill eye drops among other simple procedures (Audrey Ronning Topping, personal communication).
Rev John Lowe the secretary of the Edinburgh Medical Missionary Society in the nineteenth century wrote a handbook on the place and power of medical missions, first published around 1903. Therein he set out some of the requirements for a successful mission. First of all, the missionary’s professional education should be thorough and comprehensive. He emphasized the need for surgical training, pointing out that “natives almost everywhere have a kind of intuitive knowledge of the medicinal virtue of indigenous plants and although they are as a rule, utterly ignorant of the diseases they presume to treat, yet much confidence is placed in the native doctors and their nostrums, and, somehow they do at times appear to effect wonderful cures; but they can do nothing whatever in surgery, even in the simplest cases” [13]. Rev Lowe eschewed any private practice as a means to improve the circumstances of medical men, nor should they be paid more than ordinary missionaries, ideas that were generally not well received. Fluency with the native language was a prerequisite and having overcome that obstacle, the medical missionary should open a dispensary in as central a locality as possible, “associating himself with an earnest, intelligent, judicious native evangelist.” Patients could then be followed up in their homes by the associate. Lowe goes on to say; “Two or three intelligent native Christian youths should as soon as possible be selected and trained as assistants. They will soon be able to dispense medicines, serve as dressers and do all the drudgery of dispensary work and thus much of the medical missionary’s time will be set free for more important duties.” A hospital, on a small scale, perhaps for 2–3 patients only was to be opened as soon as possible.
Later on Lowe remarks on the practices of women “doctors” of the Madi or Moru tribe of Central Africa. These women treated all cases except wounds, accidents, and snake bites (left to male doctors). Management was the same for most diseases: a double magic wand about a foot long, one part filled with small stones and the other empty was waved and rattled over the affected part accompanied with incantations. The lady “doctor” then placed her hand into the empty tube and extracted the disease [14]. Several other spells were also commonly used and predictions made as to whether the patient should live or be killed. Séances often terminated in convulsions for the healer who upon recovery collected her fee, usually of a small domestic animal.
It is not difficult to see that many areas of the world would welcome practitioners with some better grounding in medical matters and improved chances of success. A few of the early medical missionaries and the work they accomplished are mentioned:
John Thomas
In 1793, Dr. John Thomas who had already been in Calcutta was in England seeking funds for a return mission to India. He met William Carey, known as the “father of modern missions.” Carey was one of the founders of the Baptist Missionary Society and as a missionary in the Danish colony, Serampore, India, he translated the Bible into Bengali, Sanskrit, and numerous other languages and dialects. The two travelled to India together where they established the first Protestant mission [15].
John Scudder
Dr. John Scudder, the first American medical missionary, went to Ceylon in 1819 and later travelled to India. Apart from providing medical care, he established schools and a college. He had seven sons, many of them also physicians who served as medical missionaries. His granddaughter, Dr. Ida Sophia Scudder, became a third-generation American medical missionary in India of the Reformed Church in America [16] (Fig. 1.4). She dedicated her life to the plight of Indian women and the fight against bubonic plague, cholera, and leprosy. In 1918, she started one of Asia’s foremost teaching hospitals, the Christian Medical College and Hospital, Vellore, India.
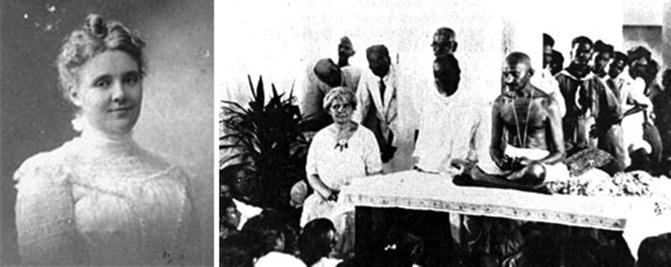
Fig. 1.4
Ida S. Scudder as a young Woman (accessed from Wikipedia March 12th 2014) and later with Mahatma Gandhi
Peter Parker
In 1834, The American Board of Commissioners for Foreign Missions sponsored Dr. Peter Parker to travel to China in 1834 where he had the distinction of being the first full-time Protestant medical missionary [17] (Fig. 1.5). Trained as a surgeon at Yale Medical School and ordained as a Presbyterian minister also at Yale, he performed many of the first surgical procedures in China. In 1835, he opened the Ophthalmic Hospital in Canton, which later became the Guangzhou Boji Hospital (the Canton Hospital). Although Parker specialized in diseases of the eye, including cataracts, and also resected tumors it soon became apparent that many other maladies required care. Over 2,000 patients were admitted the first year. Parker also introduced Western anesthesia in the form of sulfuric ether and instructed Chinese students before the establishment of medical schools. Later, Parker served as the main interpreter and negotiator of the Treaty of Wanghia with the Qing Empire. In 1845 he became a secretary and interpreter to the new embassy from the United States, while still keeping the hospital in operation. It was said that Parker “opened China to the gospel at the point of a lancet.”
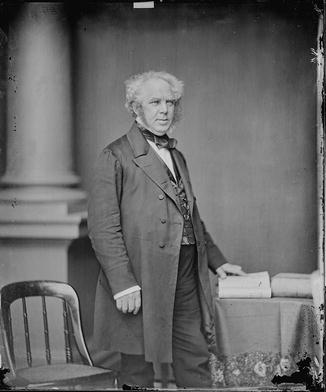
Fig. 1.5
Dr. Peter Parker, photograph by Mathew Brady (this is a file from the Wikimedia Commons. Accessed March 12, 2014)
Asahel Grant
The first American missionary to Persia and Turkey was Dr. Asahel Grant [18]. Born in Marshall, New York in 1807, he seemed to be destined to be a farmer, before slicing his foot with an axe. After a stint teaching in a country school, he studied medicine with Dr. Seth Hastings in Clinton, New York. His further medical training included auditing a chemistry class at Hamilton College and a few medical lectures in Pittsfield, Massachusetts. He did not receive a formal college degree. Despite the establishment of several medical schools by the early nineteenth century, most “doctors” assumed the title after apprenticeship to local physicians and may never have attended any medical lectures. In Utica Dr. Grant became involved with the Presbyterian Church and also set up practice as a general practitioner. In 1835, at the age of 27, and sponsored by the American Board of Commissioners for Foreign Missions he sailed with his wife, age 20 and also a missionary, to the Middle East. Within days of arrival he became ill with cholera, a disease from which he never fully recovered. Nevertheless, both he and his wife were able to build up a stellar reputation for the quality of medical care they provided and for the many schools they opened and supervised. Sadly his wife and twin children died of malaria within 5 years. He continued his work, both in providing medical care and in his many attempts to convert the Nestorians (Assyrians), a fierce isolated people who lived in the mountains of Hakkari across the border in Ottoman Kurdistan. He died of malaria and cholera in 1844 at the age of 37. His success as a physician not only saved his life on several occasions (he travelled with a lancet and bled himself frequently, treatment believed to be beneficial at that time), but opened the way for missionary successors.
Paul Brand
Only towards the end of the nineteenth century did some Protestant denominations start to provide some basic medical training for missionaries before they left their native countries. Not infrequently, these people were the only “doctors” available in the areas to which they were assigned. Dr. Paul Brand’s parents were missionaries in India and with little training and very limited supplies, for many years they were the only source of care for many remote villages. Brand, himself, was born in India in 1908 where he sustained frequent bouts of dysentery and malaria [19]. Back in the United Kingdom, he received 12 months of medical training and then returned to India as a builder. During the second World War, he studied medicine at the University College Hospital in London and as a surgeon, went back to India where he pioneered reconstructive work in leprosy, especially tendon transplants.
Nurses and Medical Missions
Undoubtedly the best known nurse in medical missions is Florence Nightingale (Fig. 1.6). Born to a very wealthy family in Florence, Italy in 1820, she resisted her family’s efforts to require her to conform to their gentrified ways. Rather she persisted in her desire to study nursing. A celebrated social reformer and statistician, and the founder of modern nursing, she came to prominence when she was sent to serve as a nurse during the Crimean War [20]. With 38 volunteer nurses that she had trained and 15 nuns she went to Scutari, a large and densely populated district and municipality in Turkey, where the death rate from cholera, typhoid, and typhus was ten times that of battle wounds. Enlisting the help of the British Government she was able to reverse these statistics and, on her return to England, set standards for hospital management and nursing care, emphasizing the use of pie charts as a visual means to understand data [21]. She established the Nightingale Training School for nurses at St. Thomas’ Hospital in 1860.
Fig. 1.6
Florence Nightingale and the medal she received from Queen Victoria (from Wikipedia; accessed March 13th 2014)
Apart from or as an extension of her ideas of social reform, Nightingale was as early promoter of medical tourism. During 1856, she sent several letters back to her family and friends in the United Kingdom describing spas in the Ottoman Empire. She had interviewed and overseen the care of several patients in these facilities and was impressed with the excellent health conditions, physical plants, general well-being, and dietary care. She noted especially that the treatment was much less expensive than in Switzerland where rich families tended to send their members, often for the care of tuberculosis. She opened the Nightingale Training School at St. Thomas Hospital on 9 July 1860. A few years later, she mentored Linda Richards, who was to be recognized as “America’s first trained nurse,” and enabled her to return to the United States with adequate training and knowledge to establish her own, high-quality nursing schools. Linda Richards went on to become a great nursing pioneer not only in the United States but also in Japan.
Related posts:
 The Evolution of Surgical Humanitarian Missions
Management of Pain in Less Developed Countries
Trauma, War, and Managing Vascular and Orthopedic Injuries
The Evolution of Surgical Humanitarian Missions
Management of Pain in Less Developed Countries
Trauma, War, and Managing Vascular and Orthopedic Injuries
 What Do Patients and Communities Expect of a Medical Mission?
What Do Patients and Communities Expect of a Medical Mission?
 Legal and Ethical Issues in Global Health: A Trip Through the Vagaries of Truth and Culture
Legal and Ethical Issues in Global Health: A Trip Through the Vagaries of Truth and Culture
 Anesthesiologists’ Role in Disaster Management
Anesthesiologists’ Role in Disaster Management

Full access? Get Clinical Tree


