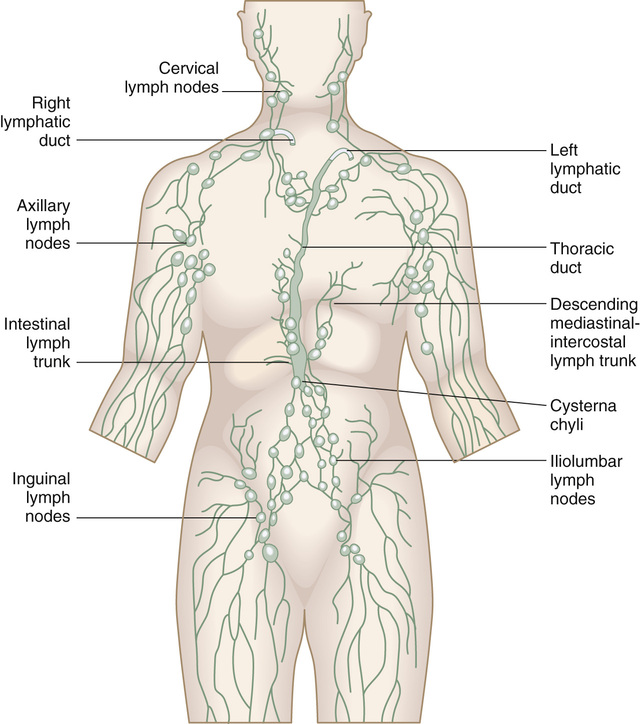
Michelle Freshman Lymphadenopathy refers to lymph nodes that have enlarged or changed in consistency. Lymph nodes typically vary from 0.5 to 2.5 cm ( On routine physical examination, generalized lymphadenopathy is a common incidental finding. A community-based sample of 2556 Dutch respondents revealed that 0.6% had unexplained lymphadenopathy, three quarters of which was localized and treated without further workup.2 Whereas the majority of neck masses in younger patients are associated with infection and are self-resolving, congenital malformations and neoplasms manifest similarly. Nodes vary in size depending on location. Epitrochlear nodes larger than 0.5 cm or inguinal nodes larger than 1.5 cm are thought to be aberrant; nodes larger than 2 cm warrant prompt investigation, although most are infectious.1 However, these enlargements become more suspicious in older patients. Malignant disease has been reported to occur in less than 1% of primary care cases of unexplained lymphadenopathy.1 The commonly cited “rule of 80s” refers to patients older than 40 years who are seen with a neck mass: 80% of all nonthyroid neck masses are malignant, and 80% of those are metastatic. Among asymptomatic cervical lumps, about 12% are head and neck cancer cases, and of these cancers, approximately 80% are squamous cell carcinoma.1 Diffuse lymphadenopathy in at-risk individuals of any age should prompt consideration of human immunodeficiency virus (HIV) infection (see Chapter 230). The lymph nodes are integral to the lymphatic drainage system and provide filtration of foreign substances through the action of lymphocytes, monocytes, and macrophages. Lymph fluid intermediates between blood and tissue. Lymph nodes are located in clusters around the lymphatic veins, where excess interstitial fluid is accumulated, processed, and returned to the bloodstream. The role of the lymphatic system in maintaining fluid balance, processing lipids and fat-soluble substances from intestinal lymph, and serving as a host defense has been a focus of therapeutic interest.3,4 More than 600 lymph nodes exist in the human body. Tonsils, adenoids, the spleen, thymus, and Peyer patches of the ileum are also involved in immune surveillance and activation. The lymphatic system is made up of head and neck (internal and external drainage), supraclavicular, deltopectoral, axillary, epitrochlear, inguinal, and popliteal regions (Figure 226-1). Because development of the lymphatic system is linked to venous development, the lymphatic ducts run along venous tracts. Lymph fluid ultimately reaches one of two large ducts in the thorax. The right lymphatic duct drains lymph from the right upper body—mediastinum, lungs, and esophagus—and into the right supraclavicular vein; the thoracic duct drains lymph from the rest of the body, including the abdominal cavity (stomach, gallbladder, and pancreas) and urogenital organs, into the left supraclavicular vein. Lymph nodes swell in response to antigens. Afferent vessels carry the antigen-laden lymph fluid into the sinus of the node; efferent vessels carry the immune-mediated fluid away. Nodal swelling is caused by the proliferation of monocytes (the precursors to macrophages). Along with the lymph nodes, other lymphoid organ tissues—including the bone marrow, tonsils and adenoids, and spleen—may become disturbed or enlarged in the presence of antigen. Splenomegaly associated with lymphadenopathy may reflect lymphocytosis generated by infection, various types of immune hyperplasia, macrophage proliferation, or a tumor. Generalized lymphadenopathy may indicate systemic disease or malignant disease because the lymph system can be infiltrated by malignant cells and other cells not normally present in the nodes. Researchers suspect that if malignant cells were prevented from entering the lymphatic system or if their microenvironment were disrupted, lymph-based cancer cells might not circulate and metastasize.3,5 In summary, lymph nodes enlarge as a result of allergy or hypersensitivity to drug or environmental pollutants, tissue injury, autoimmune disease, infection, lymphoproliferative or myeloid abnormalities of bone marrow, and other malignancies or solid tumors. Key factors to consider in the evaluation of the patient with lymphadenopathy are the age of the patient, the location of the swollen glands, and any associated symptoms. A thorough symptom analysis should reveal infectious contacts or exposures (e.g., deer ticks, bird droppings, and cat or rat feces), foreign travel, travel to endemic infectious areas, or foreign birth. Patients should be asked about possible occupational exposure to chemicals, livestock, asbestos, silica (silicon dioxide), or beryllium. Sexual behaviors should be noted. Patients should also be asked about past medical or surgical history of abdominal, thoracic, breast, head and neck, pelvic, reproductive organ, or lower extremity malignant neoplasms including those associated with acquired immunodeficiency syndrome (AIDS), surgery, or injury; implanted silicone products (e.g., breast) or prosthetics; tattoo dyes; exposure to ultraviolet radiation; personal or family history of cancer, particularly lymphoma; irradiation; and chemotherapy. A review of systems should include all areas of the skin for irregular or nonhealing lesions. A history of scalp pruritus (e.g., seborrheic dermatitis, scabies infection), conjunctivitis, eye pain, photophobia, visual complaints, unilateral ear pain, difficulty hearing, nose or throat pain or discharge, odynophagia, impaired swallowing, acidic food intolerance, vocal changes or persistent hoarseness, mastoid swelling or pain, dental maladies, dental malocclusion, facial paralysis, and muscle strain of the head or neck should be obtained elicited. Pain associated with the rapidly growing node is usually a good sign because it points to infection but may represent bleeding into the necrotic center of a malignant node.6 Breast changes, especially with axillary adenopathy, can be ominous. Lactation status should be ascertained. Gastrointestinal symptoms suggestive of malabsorption, complaints of diarrhea or constipation, or back pain with relief in the fetal position can suggest a malignant intra-abdominal process. New medications as well as long-term prescriptions are worth reviewing for potential drug hypersensitivities. Drug hypersensitivity to phenytoin sodium, carbamazepine, aspirin, hydralazine (a lupus-like mimic), allopurinol, or antibiotics (including erythromycin, penicillin, and sulfa products) and serum sickness from vaccinations to smallpox or typhoid can result in generalized lymphadenopathy. Typically drug reactions produce generalized lymphadenopathy, accompanied by rash, fever, and joint pain.1 Inquiry into the incidence and frequency of blood transfusions, sexually transmitted diseases, smoked or chewed tobacco, and illegal drug or alcohol abuse is also necessary. Use of tobacco and alcohol together increases the risk of head and neck cancer substantially. Any signs of external or internal bleeding, such as hemoptysis, hematuria, melena, or menorrhagia, should be pursued to exclude malignant disease. The history and location of the lymphadenopathy guide the physical examination (see Figure 226-1). Differentiation of normally palpable periauricular, cervical, axillary, and inguinal lymph nodes from enlarged nodes can be subtle. The nodes should be characterized by size, distribution, degree of fluctuance, firmness, matted or shoddy quality, mobility or immobility, and tenderness or nontenderness. Unilateral or bilateral involvement, hard and fixed position, and symmetry or asymmetry may indicate or exclude malignant disease. Node characteristics, whether symptomatic or painful, may not initially reveal the diagnosis, even in cases of cancer. A swollen node that is warm, tender, and rapidly enlarging may represent lymphadenitis and is suggestive of an infection at the drainage terminal. Lymphedema is an interruption of and blockage in drainage and may result from a variety of causes. Primary lymphedema refers to congenital malformations; secondary lymphedema refers to traumatic injury resulting from cancer obstruction, irradiation, recurrent infection, or surgery. Evaluation of cervical nodes requires complete muscle relaxation and neutral positioning. Both anterior and posterior cervical node enlargement can indicate infection or carcinomas of the head or neck. The presence of posterior cervical adenopathy more often suggests an infectious cause. A supraclavicular node (sentinel node) can be elicited by the Valsalva maneuver in thin individuals. The Virchow node is the left supraclavicular node, at the base of most of the body’s lymphatic drainage via the thoracic duct; an enlarged one poses significant concern for malignant disease of the stomach, gallbladder, kidney, pancreas, ovary, testes, or prostate. The right supraclavicular node drains from the mediastinum, lungs, and esophagus. Axillary nodes are terminal lymph drains for the upper extremities and can become enlarged as a result of cellulitis of the arm or hand or breast malignant neoplasms. Women with a positive axillary node require a careful breast examination and mammography to exclude breast cancer. Liver and spleen examinations looking for enlargement or tenderness are essential. Inguinal or retroperitoneal nodes may be difficult to palpate unless they are grossly enlarged. Unilateral or bilateral presentation is an important consideration because the unilateral presentation is more often malignant. Men can be seen with unilateral malignant lymphedema of the leg in cases of disseminated prostate cancer. The most likely cause of lymphadenopathy is often revealed by the history and physical examination. However, in those cases where the cause is not evident, a period of 3 to 4 weeks of observation is recommended. Often during this time a cause is revealed or a direction for further investigation is apparent. Routine diagnostics to exclude infectious disease may lead the investigation: complete blood count (CBC) with differential and enzyme-linked immunosorbent assay or Western blot HIV testing if indicated by history. Further testing, which can be extensive, is directed by the results of initial screening and by the history and physical examination findings. The diagnostics box provides a comprehensive list of studies that may be ordered, usually in consultation with a specialist. Splenomegaly with lymphadenopathy is an unusual and more ominous finding that might correlate with an abnormal CBC. Thyroid studies are warranted in suspected cases of thyroiditis, goiter, or carcinoma. Inguinal node enlargement most often has an infectious cause, and a host of sexually transmitted diseases would be part of the workup, including herpes simplex virus, gonorrhea, syphilis, chancroid, lymphogranuloma venereum, HIV, and reproductive organ cancers. A chest radiograph is necessary to rule out tuberculosis (especially in HIV/AIDS patients or those born outside the United States), sarcoidosis, infection, and local or disseminated malignant disease. A mammogram is recommended when there is a persistent axillary node enlargement without other explanation. Ultrasound is thought to be a necessary tool to assess cervicofacial lymph nodes; in fact, it is considered superior to computed tomography (CT) scan in detecting small nodes and can differentiate between solid and less concerning cystic lesions.7 CT, magnetic resonance imaging (MRI), and positron emission tomography (PET) may also contribute to diagnosis, biopsy precision, and tumor staging, particularly in the abdomen, pelvis, and chest.1 Biopsy should be considered when lymphadenopathy has persisted for more than 1 month without explanation or when malignant disease is suspected. The algorithms for selection of fine-needle aspiration cytology (FNAC) and high-tech imaging have become increasingly complex. Fine-needle aspiration (FNA) biopsy can be both highly sensitive and specific. Other techniques include ultrasound-guided FNAC and endobronchial ultrasound-guided transbronchial needle aspiration for hilar lymphadenopathy or transesophageal ultrasound-guided FNAC. Core needle biopsy may be preferable to FNAC, if it can be guided by ultrasound or CT. Surgical biopsy rather than ultrasound guided FNAC, may help with suspected lymphomas of the head or neck, given the architectural complexity of those cancerous nodes.8 Inguinal nodes have the lowest yield; supraclavicular nodes have the highest.6 With a plethora of immunohistochemical staining, flow cytometry, cytogenetics, and molecular genetic techniques available, refined diagnosis and management is ever more possible, particularly of the hematologic malignancies. Laparoscopic lymph node biopsy is preferred to all percutaneous sampling.6 Sentinel node biopsy with blue dye and radioisotope in breast cancer is considered indispensable. Typing, clinical staging, and initial management of leukemias (see Chapter 239), lymphomas (see Chapter 240), and solid tumors require a specialist. Diagnostics Lymphadenopathy Laboratory Heterophil antibody (Monospot)* HIV polymerase chain reaction (PCR)* Rapid plasma reagin or Venereal Disease Research Laboratory (VDRL) testing* Purified protein derivative (PPD) or tuberculin skin test* Cytomegalovirus PCR (urine, saliva culture or serology)* Trypanosoma serology, possible cerebrospinal fluid* Blood urea nitrogen (BUN), creatinine* Thyroid-stimulating hormone (TSH)* Erythrocyte sedimentation rate (ESR)* Monoclonal proteins in serum or urine* Serum angiotensin-converting enzyme*
Lymphadenopathy
Definition and Epidemiology
 to 1 inch) in diameter, averaging about 1 cm,1 and are characterized by number, size, shape, texture, mobility, tenderness, and surrounding skin involvement. Three quarters of patients with enlarged lymph nodes have localized findings, half of which are in the head and neck.1 Nodes located above the clavicles account for the largest palpable field; axillary and inguinal regions represent far fewer. Three or more noncontiguous groups of node enlargements constitute generalized lymphadenopathy. Lymphadenitis is defined as tender, warm, erythematous nodes, and suppurative lymphadenitis includes fluctuance.
to 1 inch) in diameter, averaging about 1 cm,1 and are characterized by number, size, shape, texture, mobility, tenderness, and surrounding skin involvement. Three quarters of patients with enlarged lymph nodes have localized findings, half of which are in the head and neck.1 Nodes located above the clavicles account for the largest palpable field; axillary and inguinal regions represent far fewer. Three or more noncontiguous groups of node enlargements constitute generalized lymphadenopathy. Lymphadenitis is defined as tender, warm, erythematous nodes, and suppurative lymphadenitis includes fluctuance.
Pathophysiology
Clinical Presentation
Physical Examination
Diagnostics

Full access? Get Clinical Tree


Lymphadenopathy
Chapter 226