69 Lung Transplantation
 Historical Perspective
Historical Perspective
Lung transplantation evolved from heart-lung transplantation as a method by which donor organs could be used more efficiently. Heart-lung transplantation was first performed in 19811 and was initially the procedure of choice for diseases that are now more commonly treated by transplant using either bilateral sequential lung transplantation or single-lung transplantation. The appeal of developing the isolated lung transplant technique was improvement in donor organ utilization. Specifically, by using each of the three thoracic organs available from a single donor (i.e., two lungs and a heart), donor organ utilization can be maximized while achieving acceptable outcomes.
Single-lung transplantation was first described in 1986.2 The advantage of the procedure is that it has allowed maximal donor utilization while being associated with good patient outcomes. The single-lung procedure has historically been accepted as the procedure of choice for common transplant indications such as emphysema and idiopathic pulmonary fibrosis and is currently performed as commonly as the bilateral procedure.3
 Survival and Demographics
Survival and Demographics
Worldwide, 1200 to 1400 patients receive a lung transplant each year. Despite the yearly increase in patients on the transplant waiting list (recently nearly 4000 patients), the number of transplant procedures performed each year has been relatively stable over the past several years (Figure 69-1).3 Significant discussion and research regarding methods to expand the donor pool are ongoing,4 but until strategies to increase lung donor procurement are actually employed, the number of transplants performed each year will likely remain stable.
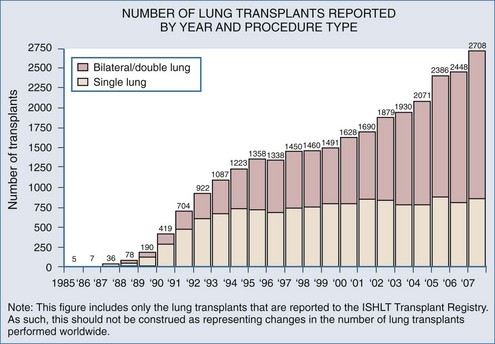
Figure 69-1 Number of lung transplants reported by year.
(Adapted from the International Society for Heart and Lung Transplantation [http://ishlt.org/]).
 Indications and Procedure Choice
Indications and Procedure Choice
Indications for lung transplant are listed in Table 69-1 according to the generally accepted procedure choice. Although there are many end-stage lung diseases that can potentially be amenable to lung transplantation, four diseases account for the vast majority of lung transplant recipients: emphysema (both cigarette-induced and due to alpha1-antitrypsin deficiency), cystic fibrosis, primary pulmonary hypertension, and idiopathic pulmonary fibrosis.3 Contraindications to transplant include evidence of extrapulmonary disease such as significant kidney, liver, or cardiac disease; poor nutritional or rehabilitation status; recent or current malignancy; and a poor psychosocial profile.
TABLE 69-1 Lung Transplant by Procedure Type (in Order of Frequency)
| Single-Lung Transplant | Double-Lung Transplant |
|---|---|
| Emphysema/chronic obstructive pulmonary disease (COPD) | Cystic fibrosis |
| Idiopathic pulmonary fibrosis | Emphysema/COPD |
| Alpha1-antitrypsin deficiency | Alpha1-antitrypsin deficiency |
| Re-transplant | Idiopathic pulmonary fibrosis |
| Primary pulmonary hypertension | |
| Bronchiectasis |
Generally the procedure of choice is the one that can be performed safely while utilizing the available donor organs most efficiently. Emphysema is the most common lung transplant indication and has consistently been associated with the best survival post transplant.3 While some controversy exists regarding the optimal procedure choice (single versus double) in this group of patients,5 most patients with emphysema who have undergone a lung transplant have received a single-lung transplant. Bilateral lung transplant has traditionally been reserved for suppurative lung diseases, such as cystic fibrosis, and other bronchiectatic disease where replacing as much infected lung tissue as possible is the primary goal. Patients with primary pulmonary hypertension generally receive a bilateral lung transplant because this prevents the potentially life-threatening situation that occurs when, in performing a unilateral transplant, nearly all cardiac output flows to the allograft, given its relatively lower vascular resistance compared to the native primary pulmonary hypertension lung. In the early transplant period when single lungs were transplanted for this indication, the result in most centers was profound unilateral pulmonary edema in the allograft.
 Candidate Selection
Candidate Selection Waiting List Considerations
Waiting List Considerations Donor Criteria
Donor Criteria
The expansion of lung transplantation as a therapy for end-stage lung disease is not limited by the number of potential recipients but rather by the availability of suitable donor organs. The standard, or “classic,” lung donor criteria are well known, if not closely followed, among lung transplant practitioners. Although some of these criteria certainly make good sense (i.e., a clear chest radiograph, no bronchoscopic evidence of aspiration), nearly all the others are controversial, often ignored, and not based on convincing research data.4 The standard or classic lung donor criteria are listed in Table 69-2. Whereas certain geographic regions in the United States, some countries in Europe, and Australia have adopted more aggressive donor management strategies that have resulted in more donor lungs, many areas with lung transplant programs have fewer than expected lung donors.
TABLE 69-2 Standard Lung Transplant Donor Criteria
PaO2 > 300 mm Hg on fractional inspired oxygen of 1.0 and positive end-expiratory pressure = 5 cm H2O |
 Postoperative Care
Postoperative Care




