Fig. 50.1
Rt L5—normal peridural fat (With permission from James Heavner)
Whether fat tissue differentiates in an alternative direction (i.e., fibrous tissue) to noxious stimuli or is replaced by abnormal pathological tissue is not known.
Vasculature
Arteries and veins traverse the epidural space. Arteries usually are small and clear. Veins usually are transparent and may be difficult to differentiate from adhesions. Arteries are easily recognizable by their pulsating behavior. Obviously, in the absence of fat, the number of visible vessels will increase. However, this may also be part of an inflammatory response. Abnormal vasculature is recognized by its increased density and chaotic orientation in areas of pathology (Fig. 50.2). Since these vessels are dilated, they contain more blood and make a strikingly purple-red appearance. Obstruction to venous blood flow leads to dilated, tortuous vessels, not only on an affected nerve root but at any site that is involved in the pathology. During epiduroscopy, some bleeding from ruptured vessels may occur; however, these vessels are often small and bleeding seems relatively insignificant.
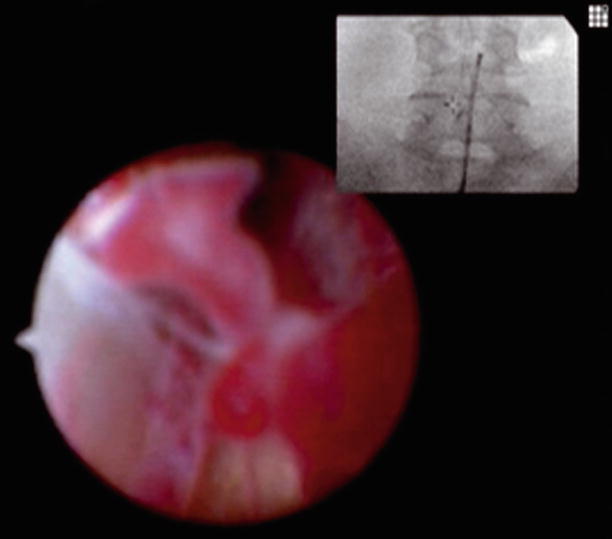
Fig. 50.2
Rt L4—hypervascularity, engorged vessels with Grade 1 fibrosis (With permission from James Heavner)
Inflammation
Inflammatory changes are common and may be part of the normal aging process. They can be found diffusely throughout the epidural space and do not seem to lead to clinical symptoms. Inflamed tissue is recognized by an ink/purple color (Fig. 50.3). It is diffuse and heterogeneous. It is the result of hyperemia and is associated with increased vasculature, exudates, and fibrosis (Fig. 50.4). If the area of inflammation is extensive or is located near the nerve root, maneuvering the scope is painful. Fragility of blood vessels in inflamed areas causes the tissues to bleed on the slightest touch with the scope. In some patients, inflammation is diffusely present in the entire lumbosacral epidural space. Total epidural fat is diminished or absent. The periosteum and dura are hyperemic, and maneuvering of the scope is painful and causes diffuse bleeding.
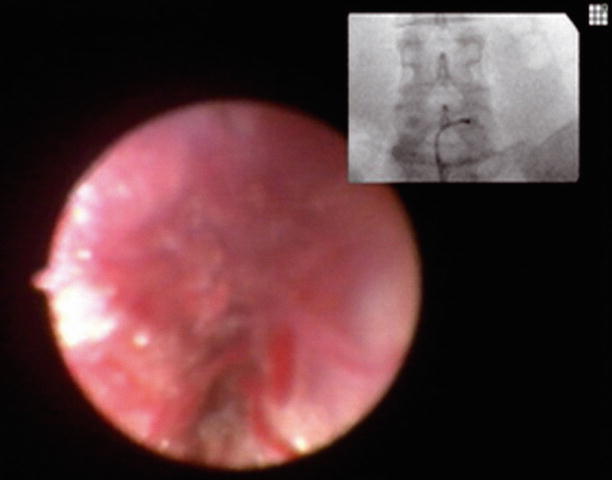
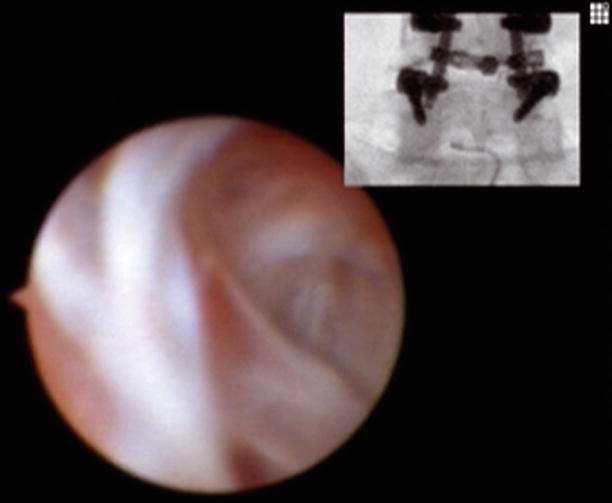
Fig. 50.3
Rt L5—active inflammation (With permission from James Heavner)
Fig. 50.4
L5 midline—active inflammation with fibrosis (With permission from James Heavner)
Fibrosis
One of the most striking images obtained through epiduroscopy is the one of white scar. Fibrosis is most likely the result of direct trauma (i.e., surgery), chronic inflammation, or local ischemia.
Independent of its cause, it is characterized by the abnormal presence of homogenous white tissue. It is typically located in the lateral recess and the neuroforamen [16]. Since epidural fibrosis may play an important role in patients with chronic back pain and radicular pain, it is useful to grade the extensiveness of the epidural fibrosis [3].
Grade I: The fibrosis consists of strings and sheets traversing the epidural space and attaching to bone or dura. It is often mixed with fat tissue and may be part of the normal aging process. It offers no resistance to advancement of the scope. Grade I fibrosis is unlikely to cause clinical symptoms.
Grade II: Strings and sheets of fibrosis increase in size and number and form a more continuous network. Inflammatory changes are often present as well. The fibrosis is starting to replace the epidural fat. There is some resistance to the scope, but the scope can still be advanced. Maneuvering the scope may be painful. It is clearly abnormal and is likely part of a pathological process that leads to clinical symptoms.
Grade III: Fibrosis is continuous and occupies discrete areas of the epidural space. There is no epidural fat and inflammation may be less pronounced. The scope cannot be advanced in these areas and attempts to do so are painful.
Grade IV: Fibrosis is now one large dense mass that is continuous and occupies an anatomical region of the epidural space (Fig. 50.5). The scope cannot be advanced at all. It is important to recognize that epidural fibrosis is associated with multiple different pathological processes and should be placed in the appropriate clinical context. For example, after back surgery, the dura may adhere to the walls of the spinal canal and be covered by strings and sheets of fibrosis. In this case, the scope cannot be advanced due to dural adhesions. This may look like a dense mass of fibrosis, but it is not. Large disc herniations may also appear as a white irregular fibrotic (grade IV) mass that are impossible to penetrate with the scope. This may be extruded disc material or a fibrotic response to chronic inflammation.
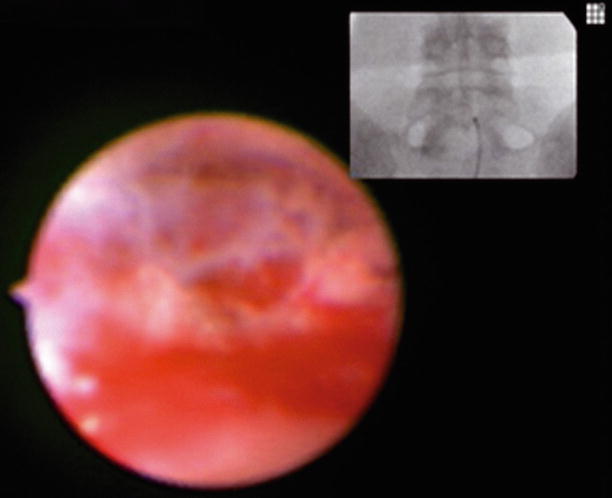
Fig. 50.5
Lt L–S junction—dense (Grade 4) avascular fibrosis (With permission from James Heavner)
Nerve Roots
Nerve roots are surprisingly hard to find for structures that occupy 30 % of the neuroforamen. The S3, S4, and S5 nerve roots are usually missed completely. This may explain why damage to these structures is rare. The S2 nerve root is easier to find, as it is larger in size. The S1 nerve root can be found in the lateral recess of the sacral epidural space on its way to the sacral neuroforamen. It passes medial and inferior to a bony structure equivalent to the pedicle of the lumbar vertebra. This is commonly the site of fibrosis and may explain persistent radicular pain in the S1 distribution after a L5/S1 fusion of the lumbar spine. The lumbar nerve roots can be found below and medial to the pedicle, the perpendicular space. A characteristic blood vessel accompanies the nerve root and can be seen through the root sleeve. Under normal conditions, this vessel is straight; with pathology it becomes dilated and gives an effaced appearance. A tortuous vessel may be a sign of circulatory obstruction. The nerve root sleeve itself can make a large dilated appearance. Touching a healthy nerve root is not painful although a paresthesia may be felt. However, in the case of pathology, touching the nerve with a scope is often very painful.
Discs, Dura, and Ligaments
As mentioned earlier, disc and disc material is difficult to identify. On gross examination, i.e., during surgery, the disc is easily identified by its white almost yellow appearance in contrast to the darker brown vertebral bone. It is only partially covered by the longitudinal ligament. The disc can probably be seen during epiduroscopy by placing the scope in the neuroforamen just superior to the pedicle; however, color, texture as seen through the scope, and, in addition, the presence of obscuring epidural fat make it difficult to obtain useful information with respect to disc pathology. A known disc herniation is characterized by the absence of epidural fat and the inability to place the scope in the neuroforamen. A dense white mass obstructs the advancement of the scope. Areas of inflammation and fibrosis may be seen as well. One does not see a nice smooth, possible red disc protrusion (compressing a nerve root) as shown in textbook pictures.
The dura is recognized by its white smooth appearance. It may pulsate with changes in CSF pressure. Blood vessels can be seen on the dura as may be fibrotic structures, possibly ligaments. In pathology, numerous areas of increased vasculature, hyperemia, and fibrosis cover the dura. These areas of inflammation may be continuous with inflammation that accompanies the nerve root. Manipulation of the scope is usually painful.
Peridural Membrane
Technical Aspects of Epiduroscopy
The Scope
We use an epiduroscope marketed by Karl Storz (Figs. 50.6 and 50.7). The usual equipment for endoscopic procedures and any flexible fiberoptic endoscope may be used as long as the images are of reasonable quality.

Fig. 50.6
Epiduroscope flexible, 2.8 mm, 40/70 cm long marketed by Karl Storz Endoskope, Tüttlingen (With permission from Danilo Jankovic)
Fig. 50.7
Materials (With permission from Danilo Jankovic)
The Procedure
At this time only one acceptable route of insertion of the scope, placement through the sacral hiatus is recommended (Figs. 50.8 and 50.9). With appropriate application of local anesthetics, the procedure can be performed without the help of an anesthesiologist. However, because of the nature of the procedure, the requirement of endoscopy, and fluoroscopy equipment, we perform the procedure in the operating room under monitored anesthesia care. Prophylactic treatment with an antibiotic may be considered. The patient is put in the prone position in such a fashion that the lumbar lordosis is minimized. The sacral area is cleansed and the skin anesthetized; an 18-G needle is advanced through the sacral hiatus in the sacral epidural space. With the assistance of fluoroscopy, a Seldinger technique is used to place a nine- or ten-French introducer in the epidural cavity.










