Lower Extremity Multiple-Stimulation Techniques
Andrea Casati
The lower limb is innervated by two plexus: the lumbar and the sacral. Among the nerves that emerge from these plexus, the sciatic nerve, which divides into the tibial and common peroneal nerves; the femoral nerve, which divides into seven terminal branches including the saphenous nerve (Fig. 14-1; [1]); and the nerve to the vastus intermedius muscle (Fig. 14-1; [2]) and the nerve to the vastus lateralis (Fig. 14-1; [3]) may be blocked using a multiple-stimulation technique. As discussed in Chapter 8, the use of a multiple-stimulation technique allows one to minimize the volume of local anesthetic required to produce surgical anesthesia. This is especially important for lower limb blocks because both a block of the femoral and sciatic nerve are required, which results in an increased risk of local anesthetic toxicity due to overdosing when the single-stimulation technique is used. Another important advantage of the multiple-injection technique is the reduced toxicity associated with intravascular injections of local anesthetics. Thus, it is well known that a negative blood aspiration before the injection of local anesthetics—although necessary—does not prevent the risk for unintentional intravascular injection.
It has been reported that withdrawing and redirecting the stimulating needle to elicit multiple motor responses might result in slightly more discomfort to the patient. For this reason an appropriate sedation with small doses of benzodiazepine combined with appropriate analgesia with opioids is indicated with the use of multiple-stimulation techniques. To minimize the risk of intraneural injection, it is important that patients remain able to report any pain during the local anesthetic injection. For this same reason, lower extremity blocks should also be performed only after the complete resolution of neuroaxial blocks.
A. Multiple-Stimulation Technique to Block the Femoral Nerve
To perform a femoral nerve block using a multiple-stimulation technique, three different muscular stimulations should be elicited: (a) the contractions of the vastus medialis, induced by stimulation of the vastus medialis/saphenous nerve; (b) the contractions of the vastus intermedius muscle with movements of the patella, induced by the stimulation of the vastus intermedius nerve; and (c) the contractions of the vastus lateralis muscle, induced by stimulation of the vastus lateralis nerve.
To minimize the risk for arterial puncture, the initial insertion of the needle should be the closest to the femoral artery. Thereafter the needle is redirected laterally.
The contraction of the vastus lateralis muscle is often associated with residual movements of the patella and sometimes can be only seen distally at the level of the knee.
Very often, the contraction of the vastus lateralis is preceded by a contraction of the sartorius muscle. To obtain the desired motor response, the needle needs to be introduced slightly deeper.
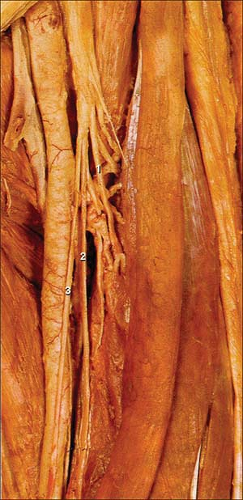
Figure 14-1. Saphenous nerve. (1) Vastus lateralis nerve; (2) Vastus medialis nerver; (3) Saphenous nerve.
In contrast to a three-in-one perivascular block, the multiple-stimulation technique to block the femoral nerve does not allow the possibility of also blocking the lateral femoral cutaneous nerve and the obturator nerve. If these blocks are required, they need to be performed individually.
With this technique, a complete sensory and motor femoral block occurs within 20 minutes.
B. Multiple-Stimulation Technique to Block the Sciatic Nerve
The sciatic nerve block produces motor responses that vary according to the level at which the nerve is being stimulated. At a high level (parasacral, posterior, and sub-gluteal), three types of responses are elicited: (a) the dorsiflexion or eversion of the foot, induced by the stimulation of the common peroneal branch of the sciatic nerve; (b) the plantar flexion of the foot and toes produced by the stimulation of the tibial branch of the sciatic nerve; and (c) the contraction of the biceps femoris induced by the stimulation of the branches innervating the hamstring muscles. Above the knee (lateral and posterior popliteal nerve block), only contraction of the foot and toe muscles are observed. Although the sciatic nerve divides into the common peroneal and tibial nerves above or at the popliteal fossa, the two branches can be clearly identified from its origin; and in about 10% of cases they are two separate nerves already at the ischiatic foramen. Nevertheless, and except in amputated limb cases, the distal motor responses (dorsiflexion or eversion) and flexion of the foot and toes are searched to block the common peroneal and tibial nerves, respectively.
Related posts:






Full access? Get Clinical Tree


