38 EPIDEMIOLOGY OF LIFE-THREATENING ASTHMA PATHOPHYSIOLOGY AND IMMUNOLOGY OBJECTIVE MEASUREMENT OF OBSTRUCTION LABORATORY AND RADIOGRAPHIC DATA NONTRADITIONAL THERAPY OF SEVERE BRONCHOSPASM ACUTE SEVERE ASTHMA IN PREGNANCY MECHANICAL VENTILATION IN ASTHMA PATIENTS Worldwide an estimated 300 million people suffer from asthma and this number is estimated to grow by more than 100 million by 2025. About 70% of asthmatics have allergies and 11% of cases are related to workplace conditions such as exposure to fumes, gases, or dust. Older asthmatic patients (≥60 years) tend to have severe or near-fatal asthma exacerbation compared to younger asthmatics (<60 years).1–4 Common triggers for acute asthmatic attacks include air pollutants, respiratory tract infection, and allergen exposure. An association of panic-type anxiety and life-threatening asthma has been suggested. Box 38.1 contains a comprehensive list of precipitating factors. In the 1960s, a global alarm was sounded when sharp epidemic increases in asthma death rates were reported. Deaths approximately doubled in the United States from 1980 to 1995. After a long period of steady increase, asthma mortality and morbidity rates have continued to decline for the past decade.3,5–7 In patients 5 to 44 years old, death from asthma peaks in the summer months, although hospitalizations peak during the winter months. In older asthmatic patients, a different distribution is seen, with hospitalizations and mortality rates both peaking in the winter months. Older patients with asthma also have been shown to have fewer symptoms of dyspnea with methacholine-induced obstruction.8 Polynesians, African Americans, and black South Africans all have been reported to have higher asthma mortality rates. Likely reasons include genetic predisposition or poor management of severe asthma attacks because of reduced or delayed use of health care services and lower level of understanding. Self-medication also may play a role. Pendergraft and colleagues9 reported that among 29,430 admissions in the United States with a primary diagnosis of asthma, 10.1% were admitted to intensive care units (ICUs), and 2.1% were intubated. The risk of in-hospital death was significantly higher in patients who were intubated and who had comorbid conditions. Near-fatal events occur in 2% to 20% of patients admitted to ICUs with acute severe asthma and in 2% to 4% of those intubated for respiratory failure. Risk factors for death from asthma are previous severe exacerbations with ICU admission or intubation, two or more hospitalizations within the past year, three or more emergency department visits in the past month, use of more than two canisters of short-acting β-agonist in the past month, and difficulty in perceiving or articulating asthma symptoms. African-American ethnicity, low socioeconomic status, urban residence, substance abuse, cigarette-smoke exposure, psychological factors (anxiety and depression), and comorbid problems such as cardiovascular diseases, chronic pulmonary diseases, and chronic psychiatric illnesses are other potential risk factors for death from asthma. The strongest predictor of mortality risk from asthma is a prior episode of near-fatal asthma, estimated to be 15% to 22%. Asthma death rates per 1000 persons with asthma were 30% higher for females than males, 75% higher for blacks than whites, and seven times higher for adults compared to children. Adults over 65 years old had the highest death rate of 0.58 per 1000 persons with asthma.9–13 About 5% of asthma patients have “difficult asthma” (asthma difficult to control with maximal recommended doses of inhaled medications, in particular, inhaled corticosteroids). Most of these patients meet the criteria for severe asthma or may have chronic mild or moderate disease with acute exacerbations. Two clinical patterns of life-threatening asthma have been reported. A more serious type is the slow onset of life-threatening asthma characterized by onset over days to weeks, copious amounts of mucoid secretions with intense eosinophilic infiltration, and resistance to bronchodilator therapy. This pattern is described as “slow onset–late arrival,” or type 1, and accounts for 80% to 85% of fatal asthma. Second is the sudden type of asthma characterized by onset over minutes to hours with acute bronchospasm, absence of large quantities of airway secretions with no mucous plugs but neutrophil infiltration of the submucosa, typically a marked response to bronchodilators, and quick recovery in most circumstances. This is described as “sudden asphyxic asthma,” or the type 2 scenario of asthma death. Sudden-type asthma accounts for about 15% to 20% of fatal asthma.14–16 Manthous and Goulding studied the effect of intravascular volume status on deadspace fraction in mechanically ventilated patients with severe asthma. They noted a mean increase in deadspace ventilation of 4.2% in response to intravascular volume expansion with 250 to 500 mL of normal saline solution.17,18 Characteristic findings of fatal asthma are airways showing infiltration with neutrophils and eosinophils, degranulated mast cells, sub–basement membrane thickening, loss of epithelial cell integrity, occlusion of bronchial lumen by mucus, hyperplasia and hypertrophy of bronchial smooth muscle, and hyperplasia of goblet cells. Asthma is an inflammatory response evidenced by the presence of cytokines that mediate inflammation and chemotactic chemokines in bronchoalveolar lavage fluid and pulmonary secretions. Some cytokines initiate inflammatory response by activating transcription factors, which act on genes that encode inflammatory cytokines, chemokines, adhesion molecules, and other proteins that induce and perpetuate inflammation. Adhesion molecules provide a mechanism for the adhesion of inflammatory cells to the endothelium and migration of these cells from the circulation into the lamina propria, epithelium, and the airway lumen itself.19 Busse and Lemanske described the immunology of allergic inflammation in asthma. IgE antibodies are linked to the severity of asthma. The release of cytokines depends on cross-linking of IgE by allergen. IgE antibodies are synthesized and released by B cells; briefly circulate in the blood; and bind to high-affinity IgE receptors on the surface of mast cells in tissues and peripheral blood basophils and low-affinity IgE receptors on lymphocytes, eosinophils, platelets, and macrophages.20 The early phase of asthma (usually resolves within 1 hour) is characterized by an inhaled allergen precipitating acute constriction of smooth muscles by release of histamines and leukotrienes from mast cells. A prolonged late phase (4 to 6 hours later) occurs as a result of cytokines and chemokines generated by resident inflammatory cells (mast cells, macrophages, epithelial cells) and recruited inflammatory cells (lymphocytes, eosinophils) and causes further obstruction of airflow. Numerous cytokines regulate the function of eosinophils and other cells in asthma. Interferon-γ is elevated in severe asthma during the acute phase. Data also suggest that interferon-γ contributes to the activation of eosinophils and likely augments inflammation. There are two types of helper CD4+ T lymphocyte cells. Type 1 helper (TH1) T cells produce interleukin (IL) 2 and interferon-γ, which are essential for cellular defense mechanisms. Type 2 helper (TH2) T cells produce cytokines (IL-4, IL-5, IL-6, IL-9, and IL-13) that mediate allergic inflammation. Balance between the TH1 and TH2 type cytokine response contributes to the cause and evolution of atopic diseases, including asthma. The increasing prevalence of asthma in Western countries has led to the “hygiene hypothesis.” The immune system in newborns is primarily TH2 cells, and a timely and appropriate environmental stimulus is needed to create a balanced immune response. Alteration in the number of infections in early life, widespread use of antibiotics, adoption of the Western lifestyle, and repeated exposure to allergens may affect the balance between TH1-type and TH2-type cytokine responses and increase the likelihood of immune response by TH2 cells and lead to asthma. Mild intermittent asthma is thought to be a TH2 allergen-oriented reaction with adequate apoptosis and self-limiting inflammation, although severe persistent asthma is mediated by TH1 cytokines with progressive loss of apoptosis leading to longer exacerbations, expanded memory cells, and persistent inflammation. Evidence continues to underscore the importance of immune factors in the development of asthma and resulting inflammatory process. This particular strategy and insight into the mechanisms of these processes would be important for future treatment of acute severe asthma.19,21–25 Airflow limitation in asthma is caused by bronchoconstriction, airway edema, airway hyperresponsiveness, and airway remodeling. Permanent structural changes can occur with airway remodeling, leading to poor response to therapy, including thickening of sub–basement membrane and subepithelial fibrosis, airway smooth muscle hypertrophy and hyperplasia, blood vessel proliferation and dilation (angiogenesis), and mucus gland hyperplasia and hypersecretion.13 Asthma and atopy are complex phenotypes that are influenced by genetic and environmental factors. About 79 genes have been associated with asthma or atopy phenotypes. The ADAM33 gene has been associated with asthma. A locus on the short arm of chromosome 20 has been linked to asthma and bronchial hyperresponsiveness. If further investigations confirm that ADAM33 is an asthma gene, future studies should enhance understanding of asthma and lead to new therapeutic targets. As Ober and Hoffjan described, such “molecular phenotyping” of patients with asthma and atopic diseases may generate informed decisions regarding treatment, laying the foundation for genomic medicine in the next decade.26,27 Wheezing may be expiratory and inspiratory and correlates with the degree of obstruction if adequate air movement is present. Absence of wheezing is an ominous finding in a severely distressed asthmatic patient because it implies minimal air movement and is a harbinger of respiratory arrest. Contraction of the sternocleidomastoid muscles and other accessory muscles indicates severe obstruction (FEV1 < 1 L). Intense inspiratory effort leads to large swings in intrathoracic pressure and to an accentuated pulsus paradoxus (representing a decreased stroke volume during inspiration). Pulsus paradoxus is often appreciated during routine blood pressure measurement in acute severe bronchospasm because systolic blood pressure decreases dramatically during inspiration (this decrease is <10 mm Hg in normal individuals). A decrease of more than 15 mm Hg in a patient in an acute asthma episode is associated with severe reduction in FEV1.18,28,29 Ominous signs and findings during an acute severe asthma episode include diaphoresis, inability to recline or talk, peak expiratory flow rate (PEFR) less than 60 L/minute, and use of accessory muscles. PEFR less than 25% predicted or personal best is defined as severe life-threatening asthma. In acute severe asthma, lung hyperinflation occurs secondary to increased expiratory airflow resistance, short expiratory time, high ventilatory demands, and increased postinspiratory activity of the inspiratory muscles. The presence of these factors in variable degrees does not allow the respiratory cycle to reach a static equilibrium volume at the end of expiration. Inspiration begins at a volume in which the respiratory system exhibits a positive elastic recoil pressure called intrinsic positive-end expiratory pressure (iPEEP), or auto-PEEP. This phenomenon is described as dynamic hyperinflation. Dynamic hyperinflation produces a significant decrease in systemic venous return to the heart, leading to a decrease in left ventricular diastolic filling. Also problematic is the increase in left ventricular afterload as a result of large negative intrathoracic pressure swings during inspiration. Pulmonary artery pressure also may be increased secondary to lung hyperinflation, resulting in increased right ventricular afterload. These events combine to produce pulsus paradoxus.15 Near-fatal asthma presents as raised PaCO2 requiring mechanical ventilation and is associated with high inflation pressures. Life-threatening asthma has any of the following features. Symptoms are altered mental status with confusion or coma, feeble respiratory effort, and exhaustion. Signs are cyanosis, silent chest, hypotension, bradycardia, oxygen saturation below 92% or PaO2 less than 60 mm Hg, PaCO2 higher than 60 mm Hg, and FEV1 below 30% predicted or personal best.30 All that wheezes is not asthma. Other entities to consider are upper airway obstruction and “cardiac asthma.” Upper airway obstruction should be considered in patients at risk (e.g., tracheal stenosis in patients who were previously intubated) and when there is no response to therapy in a patient without history of asthma. If the patient’s status would tolerate it, flow volume loops may be diagnostic. Likewise, wheezing that dissipates with intubation should make one suspect upper airway obstruction. Paradoxical vocal cord movement can stimulate asthma. Patients with acute left ventricular failure may wheeze as a result of interstitial fluid compression of bronchioles and edema-associated bronchiolar smooth muscle contraction.31,32 During an asthmatic attack, all indices of expiratory flow are significantly reduced, including FEV1; FEV1/FVC; PEFR; maximal expiratory flows at 75% (MEF75), 50% (MEF50), and 25% of vital capacity (MEF25); and maximal expiratory flow between 25% and 75% of the FVC (MEF25-75). With acute asthmatic crisis, high functional residual capacity, total lung capacity, and residual volume are observed.15 Although spirometry is the best objective measure of airway obstruction, a severely ill asthmatic patient is rarely able to perform the necessary full FVC maneuver. Objective assessment of airway obstruction in a severe asthmatic usually can be made by measuring the PEFR because this measurement requires patient cooperation only in the early part of the FVC maneuver. Because the greatest expiratory flow rates exist in early expiration, most patients are able to produce a reliable PEFR value. Normal expiratory flow rates vary considerably with age, sex, and height. In adults, a PEFR less than 100 to 125 L/minute implies severe obstruction to airflow. A severe exercebation of asthma is defined as an FEV1 less than 40% or peak expiratory volume, less than 40% predicted, or less than 1 L. Values less than 25% are consistent with life-threteaning asthma. Failure to improve PEFR significantly with initial aggressive bronchodilator therapy is the best predictor of morbidity in a patient with acute severe asthma.10 Asymmetrical breath sounds or chest pain should alert the physician to the possibility of pneumothorax and mandates an early chest radiograph. An increased white blood cell count may be produced by asthma alone in the absence of infection, β-receptor agonists, and theophylline shift of potassium intracellularly. Hypokalemia-induced dysrhythmias could occur after intensive bronchodilator therapy in elderly patients or in patients receiving other therapies that predispose to hypokalemia, such as steroidal and diuretic medications. Creatine phosphokinase (non-MB fraction) may be increased as a result of the strenuous activity of ventilatory muscles. Severe asthma may cause right-sided heart strain as shown on electrocardiogram; this resolves with clinical improvement. Arterial blood gas assessment adds little to the early management of acute asthma. The early stage of asthma usually reveals mild hypoxemia, hypocapnia, and respiratory alkalosis. A non–anion gap acidosis also may be observed in patients with severe asthma if several days of hyperventilation have led to renal compensation with bicarbonate wasting to compensate for the respiratory alkalosis. As the severity of obstruction increases, arterial carbon dioxide (PaCO2) normalizes and then increases as a sign of impending respiratory collapse. After initial therapy, arterial blood gases may be useful for decisions regarding hospital admission or tracheal intubation. Most asthma patients respond dramatically to initial therapy; arterial blood gases obtained when the patient is first seen are rarely predictive of outcome or useful clinically.33 Early attention should be directed toward aggressive therapeutic intervention. A normal PaCO2 level in a distressed asthmatic patient despite aggressive in-hospital therapy should alert the physician to respiratory fatigue and the danger of respiratory arrest. Respiratory acidosis may be preceded by a lactate-induced anion gap metabolic acidosis. This lactic acidosis is likely caused by a combination of failing inspiratory muscles, aggressive use of β-agonist therapy, and decreased liver perfusion resulting from increased intrathoracic pressure and blood flow diverted to the muscles of respiration. Lactic acidosis occurs more commonly in men and with administration of parenteral β-agonists.34–36 In patients with near-fatal asthma, high values for inflammation-related laboratory markers such as erythrocyte sedimentation rate (ESR), C-reactive proteins (CRP), and low nutritional status with low albumin levels were associated with poor prognosis. Exhaled nitric oxide is another biomarker of lung and airway inflammation. Elevated exhaled nitric oxide levels can be found in severe allergic asthma and may predict future exacerbations and steroid treatment response. Use of this biomarker is not recommended at this time and needs further evaluation.37,38 Conditions typically requiring hospitalization for a patient with severe asthma are listed in Box 38.2. If pulse oximetry confirms the presence of hypoxemia, oxygen should be given to maintain oxygen saturation at greater than 92%. A transient decrease in arterial oxygen tension has been shown in some patients after initiation of β-adrenergic agonist therapy in severe asthma. Mechanisms of this decrease relate to some combination of β2-agonist-induced vasodilation in areas of decreased ventilation and increase in pulmonary blood flow resulting from a β1-adrenergic inotropic and chronotropic effect. Saturation may decrease initially during bronchodilator therapy with β-agonists, which produce vasodilation and may increase intrapulmonary shunting. Studies in children suggest that aerosolized salbutamol administration may cause hypoxemia during acute episodes of asthma if the drug is administered without oxygen. Most published data show that salbutamol does not have a clinically important effect on oxygenation in asthmatic adults. This seems to be true for stable and acute asthma; however, these studies in adults exclude the most severe exacerbations more likely to be associated with marked hypoxemia. Because inhaled β-agonist should be given in this circumstance, the only clinical response is to treat any worsening of oxygenation that occurs with additional oxygen. Hyperoxia may be harmful and may be associated with hypercarbia due to regional release of hypoxic pulmonary vasoconstriction during asthma exacerbations.5,39–42 Moloney and colleagues showed that bronchoconstriction induced by dry air challenge can be prevented by humidifying inspired air. Humidification of inspired air should be achieved with a heated cascade humidifier. The use of heat and moisture exchangers is discouraged because they increase the deadspace and add to the expiratory airway resistance.43 Albuterol is the cornerstone of treatment for acute exacerbation in patients with acute asthma. Initial therapy in an acutely ill asthma patient, as recommended by the National Asthma Education and Prevention Program Update, is 2.5 to 5 mg of albuterol (0.5 to 1 mL of 0.5% solution in 5 mL of normal saline solution) by nebulization every 20 minutes for three doses (for optimal delivery, dilute aerosols to a minimum of 3 mL at gas flow of 6 to 8 L/minute), followed by 2.5 to 10 mg every 1 to 4 hours as needed, or 10 to 15 mg/hour continuously, with the titration based on response and severity of symptoms. Continuous nebulization should be considered in the most severe patients. Tachycardia and hypokalemia may occur with continuously nebulized albuterol. β2-Selective agents delivered parenterally or orally lose much of the β2 selectivity, which provides the rationale for inhalation treatment as the cornerstone of therapy.25,32,39,40,43,44 Adequate delivery of β-agonists can be accomplished by a metered-dose inhaler (MDI) with spacer during acute bronchospasm if proper technique is used and doses are increased. Four puffs of albuterol (0.36 mg) delivered with a spacer should be expected to be equipotent to 2.5 mg of albuterol by nebulization in patients with severe disease. It is advisable to deliver the β-agonist by nebulization in most acutely ill asthma patients because nebulization requires minimal coordination and cooperation of the patient and less bedside instruction and supervision by health care professionals. Many randomized controlled clinical studies over the last several decades have compared β-agonists delivered by MDIs or by nebulizer. Most studies show similar responses. Protocols typically include methods that ensure proper use of the MDI, however. Greater amounts of drug delivery are required with nebulized therapy to produce the same effect as that seen with an MDI with a spacer. To initiate therapy with nebulized albuterol and then switch to an MDI with spacer after the patient has improved and stabilized may be cost-effective. When aerosol β-agonists are delivered in intubated patients and patients receiving mechanical ventilatory support, much of the physiologic effect is lost as a result of deposition onto the endotracheal tube. Doubling the dose that would be used in a nonintubated patient is recommended.45–47 Aggressive inhaled selective β2-agonist therapy is preferred to intravenous albuterol because the same end point usually can be achieved with less risk for toxicity. Intravenous albuterol (if available) may be considered as an alternative when patients with life-threatening asthma have failed to respond to inhaled therapy. Oral β2-selective agents should not be used as primary treatment for patients with acute asthma because the therapeutic-to-toxicity ratio is less than with inhaled agents. Effects of corticosteroids and β2-agonists on airflow obstruction may be additive.48 Levalbuterol, 0.63 mg, is equivalent to racemic albuterol, 1.25 mg, for efficacy and side effects. Levalbuterol is available as 0.63 mg/3 mL and 1.25 mg/3 mL nebulizer solutions. The recommended adult dose of levalbuterol is 1.25 to 2.5 mg every 20 minutes for three doses, then 1.25 to 5 mg every 1 to 4 hours as needed, or 5 to 7.5 mg/hour continuous nebulization.25 In outpatient settings, monotherapy with inhaled long-acting β-agonists (LABA, salmeterol, Formoterol) has been shown to increase severe and life-threatening asthma exacerbations and asthma-related deaths.30 Subcutaneous β-agonist therapy has a disadvantageous therapeutic-to-toxicity ratio compared with inhaled β2-selective agonists. Although there is no proven value of systemic therapy over aerosol therapy, rapid delivery of β-agonists to the airway may be beneficial in seriously ill asthmatic patients who are at imminent risk for respiratory arrest or in need of intubation and at low risk for β-agonist cardiac toxicity (young asthmatics). In this circumstance, a combination of inhaled and subcutaneously administered β-agonists may be useful. The subcutaneous epinephrine dose for adults is 0.3 to 0.5 mL of a 1 : 1000 dilution (1 mg/mL), depending on age and weight; it may be repeated in the initial management every 20 minutes for three times. An alternative subcutaneous β-agonist agent is subcutaneous terbutaline, 0.25 mg, which can be repeated every 20 minutes for three doses. When subcutaneous terbutaline is compared with subcutaneous epinephrine, equal cardiac side effects are seen. No clinical studies document benefit of subcutaneous terbutaline over subcutaneous epinephrine. Terbutaline is, however, the parenteral agent of choice in pregnancy. β1-Adrenergic stimulators are given subcutaneously with caution to the elderly and to patients with documented or suspected coronary artery disease.49,50 Anecdotal reports have suggested the success of epinephrine administration through the endotracheal tube after respiratory arrest from asthma. Prospective trials are needed in this area. Despite the lack of confirmatory studies, in an asthma patient with respiratory arrest, it may be considered.51
Life-Threatening Asthma
Epidemiology of Life-Threatening Asthma
Triggers of Acute Asthma
Mortality Rates for Asthma
Classification
Pathophysiology and Immunology
Asthma Genetics
Symptoms and Signs
Objective Measurement of Obstruction
Laboratory and Radiographic Data
Inpatient Admission Decisions
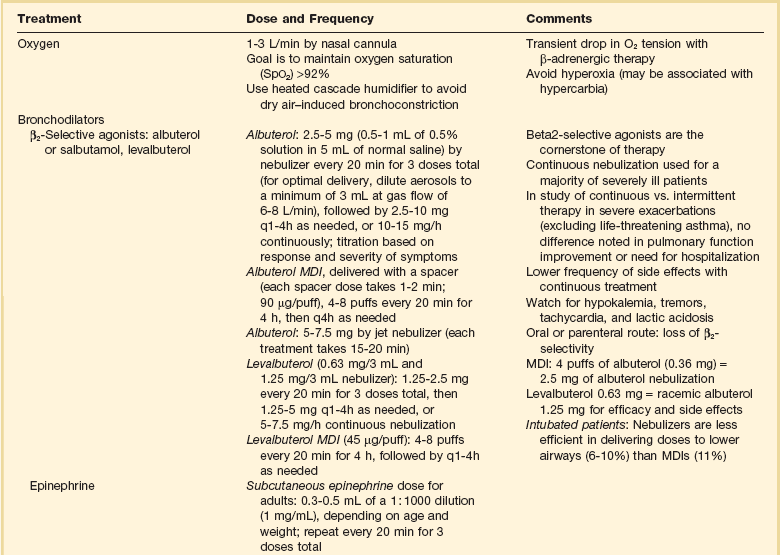
Drug Therapy (Table 38.1)
Oxygen
β-Adrenergic Therapy
Inhaled β2-Selective Agonists (Albuterol or Salbutamol) and Short-Acting β-Agonists
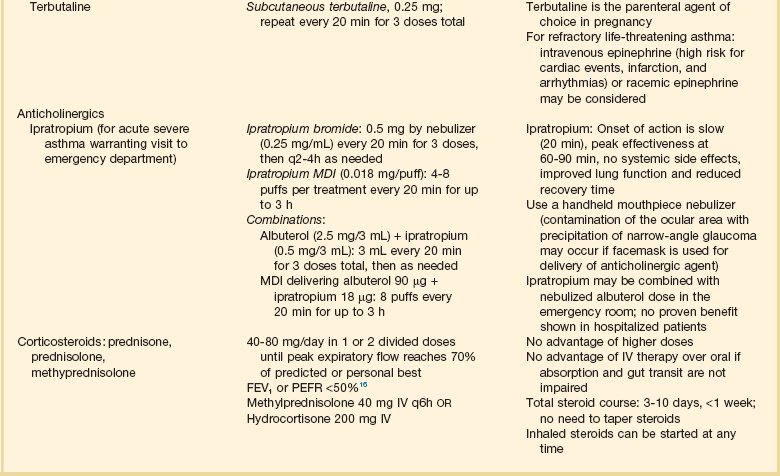
Subcutaneous β-Agonist Therapy (Epinephrine or Terbutaline)
Life-Threatening Asthma