Fig. 64.1
Schematic diagram showing the pathway of a typical course of lateral femoral cutaneous nerve. Note that the nerve courses beneath the inguinal ligament and runs superficially to the sartorius muscle and then in between this muscle and tensor fascia lata muscle (Reproduced with permission from Philip Peng Educational Series)
Fig. 64.2
Dermatome of lateral femoral cutaneous nerve (Reproduced with permission from Danilo Jankovic)
Anatomy
After forming near the lumbar spine, the LFCN emerges from the lateral border of the psoas major muscle and crosses the iliacus muscle obliquely under the fascia iliaca (Fig. 64.3). Before it reaches the level of the anterior superior iliac spine (ASIS), it crosses under the deep circumflex artery [3, 4].
Fig. 64.3
Nerves at the inguinal area (Reproduced with permission from Philip Peng Educational Series)
The LFCN usually emerges from under the inguinal ligament (IL) medial to the ASIS at a variable distance (average 29 mm; range 0–73 mm) [3, 5–7]. In patients with meralgia paresthetica, however, a recent study using high-resolution ultrasonography revealed the nerve to be closer than normal patients to the ASIS, with a mean distance of 5.2 mm (SD 4.6 mm) [6]. A few anatomical variations that one should bear in mind in scanning the LFCN: it may course over or through the IL rather than under it, it may branch before crossing the IL in up to 28 % of cases, and it may pass over or posterior the ASIS in 4–29 % of cadavers [8, 9]. The average diameter of LFCN was found to be 3.2 ± 0.7 mm [4] although there is no established normal value for cross-sectional area.
Once the LFCN passes under the IL, it usually enters the thigh superficial to the sartorius muscle confined by the fascia lata, although in 22 % of cases the LFCN may pass through the sartorius muscle [4] or at times medial to it [8]. Thereafter the LFCN is visualized in a plane between the tensor fascia lata muscle and the sartorius muscle. It will normally divide into an anterior and a posterior branch and will pierce the fascia lata in order to innervate the skin.
Sonoanatomy
The LFCN can be difficult to visualize with ultrasound since it is a small nerve, is often surrounded by connective tissue, and has a variable anatomic course. It may appear round or oval shaped and may be hyperechoic or hypoechoic or have a mixed pattern (Fig. 64.4). In many cases of meralgia paresthetica, a portion of the nerve will appear enlarged or swollen (pseudoneuroma) although this can be an incidental finding in the occasional normal patient (Fig. 64.5) [6]. In order to locate the LFCN accurately, high-resolution ultrasonography (HRUS) with 18 MHz high-frequency probes has been utilized [6, 7]. The LFCN is best visualized inferior to the ASIS in a connective tissue plane between the sartorius and tensor fascia lata. However, in order to achieve therapeutic relief of meralgia paresthetica, it is important to block the LFCN as close to the IL as possible, which is often considered the source of irritation or compression of the nerve. Thus it is important to dynamically scan a wide area when performing a LFCN block.
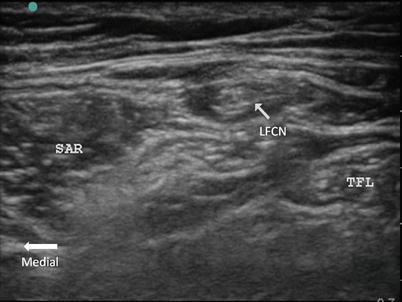
Fig. 64.4
Ultrasonographic picture showing different morphology of the lateral femoral cutaneous nerve (LFCN). It can be in form of hyperechoic or honeycomb appearance as indicated by line arrows in figure (a). The fascia is indicated by bold arrows (FL fascia lata, FI fascia iliaca); the ilium is indicated by solid arrowheads; SAR sartorius muscle; ASIS anterior superior iliac spine. The LFCN may branch into smaller nerves and appears as hypoechoic structures (solid line arrows) in figure (b) (Reproduced with permission from Philip Peng Educational Series)
Fig. 64.5



The ultrasound appearance of the LFCN in a patient with meralgia paresthetica. The nerve appears large and swollen, embedded in the adipose tissue in the grove formed by the tensor fascia lata (TFL) and sartorius (SAR) (Reproduced with permission from Philip Peng Educational Series)
Related posts:






Full access? Get Clinical Tree
