Chapter 17 Laryngoscopic Orotracheal and Nasotracheal Intubation
Our very breath, pre-language of the lingus,
Unspoken and unseen, lies all around us;
It tunnels through a darkened path to bring us
Before the guarded gates that would confound us:
Dentition, palate, epiglottic folds
Are navigated as the case is started
And followed through to cartilage that holds
The two true cords, those gleaming pillars, parted;
Here human hands, left trembling with creation,
Are re-creating life as it began,
Beginning with the step of intubation,
The God-breathed breath of life blown into man.
I A Short History of Endotracheal Intubation
Cannulation of the trachea, or aspera arteria, as it was called by Robert Hooke,1 was initially described as a technique for positive-pressure ventilation (PPV):
The use of tracheal cannulation for the administration of anesthetics and provision of a patent airway was first reported in 1858 by John Snow in On Chloroform and Other Anaesthetics,2 in which he described a tracheostomy and cannulation for the administration of chloroform in a spontaneously breathing rabbit. The first human use of tracheostomy for anesthesia and protection against aspiration was reported by Trendelenburg in 1869, and it also was accompanied by spontaneous ventilation.3 In the next 10 years, numerous investigators developed nonsurgical techniques and apparatus for cannulation of the trachea for surgical (ear, nose, throat) or medical (diphtheria) indications. Matas was among the first to advocate the use of PPV through a tracheal cannula to avoid the catastrophic consequences of pneumothorax for a spontaneously ventilating patient during thoracotomy.5
Endotracheal anesthesia came into its own during and immediately after World War I because of the volume of facial and mandibular injuries treated in England, especially at the hospital in Sidcup. In 1936, I.W. Magill wrote one of many descriptive treatises on intubation in anesthesia5:
Immediately thereafter, Magill inserts a caveat:
II Laryngoscopic Orotracheal Intubation
A Preparation and Positioning
Box 17-1 lists the basic materials required for conventional orotracheal intubation. The materials are grouped according to the temporal sequence of events. All items are required for routine intubation, dealing with common difficulties, or preventing complications. Redundancy is the key in preparing for a critical event, such as endotracheal intubation. All essential equipment (e.g., laryngoscope handles, ETTs) should have readily available back-up counterparts in case of unexpected failure. An assortment of laryngoscope blades, both straight (Miller) and curved (Macintosh), should be available.
Box 17-1 Basic Equipment for Endotracheal Intubation
The proper sequence of events before laryngoscopy should be followed:
1. Adequate access to the head of the bed or table is essential. Removal of side rails and headboard (if outside the operating room) ensures freedom of movement; confirming that the bed or table is locked in position prevents unnecessary and stress-inducing pursuit of the patient around the room. The height of the surface should be adjusted to the level of the laryngoscopist’s chest. An experienced aide should be in constant attendance to provide items such as suction lines, airways, tubes, and drugs to the primary laryngoscopist, as well as to apply optimal external laryngeal manipulation (OELM), as needed.
2. The patient must be properly positioned before laryngoscopy. Patients who are uncooperative, agitated, or otherwise mobile may require rapid and efficient positioning after sedation. Pads or rolls should be prepared in advance and be readily at hand.
The earliest attempts at laryngoscopy used the classic positioning of full extension. Described by Jackson in 1913, this position required full extension of the head and neck on a flat surface.6 After 20 years, he amended his view to one that supported the contemporary sniffing position of flexion at the neck and extension at the head.7 This was accomplished by supporting the head on a pillow that was at least 10 cm thick. Numerous investigators have examined radiographs of subjects to determine the optimal positioning for orotracheal access. Various theoretical models of positioning for intubation have been proposed. For the past 60 years, the three-axis theory has proposed that the oral, pharyngeal, and laryngeal axes should be brought into approximate alignment to best facilitate orotracheal visualization and intubation (Fig. 17-1). Proposed by Bannister and MacBeth in 1944, this model presumes that laryngoscopy is done in the midline (two-dimensional model) and that laryngeal axis alignment is necessary for proper intubation.8 This idea has been challenged by the work of Adnet and colleagues in imaging studies and clinical comparisons.9–11
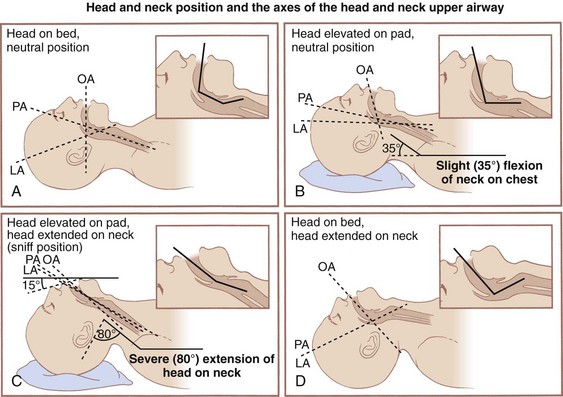
Adnet’s conclusion, however, has been questioned at length.12 Greenland and colleagues reexamined the issue, finding “the sniffing position the most favorable for direct laryngoscopy” as determined by magnetic resonance imaging (MRI).13 This perspective has been corroborated by evidence indicating 9 cm as the optimal pillow height.14 Others have advocated for an extension-extension position, in which the head and neck are extended by lowering the head of the table 30 degrees, proposing that direct laryngoscopy requires less axial force in this position than in the sniffing position.15 Whether the lower cervical spine is flexed, extended, or neutral, the extension of the atlanto-occipital joint remains the critical factor for optimal positioning. The reasonable option in view of conflicting evidence (and patients’ variability) is to position the patient with the occiput on a pad (traditional sniffing position) and be prepared to remove the pad (convert to simple extension) if the initial laryngoscopy becomes inadequate (Fig. 17-2).
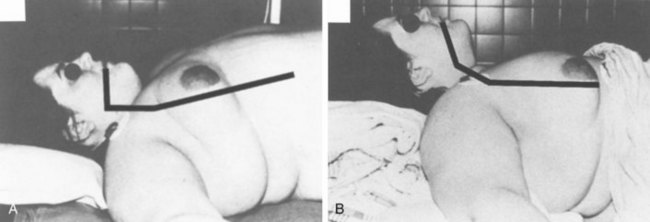
Obese patients often require more extensive padding (planking) starting at the midpoint of the back to the head to assume an optimal position for laryngoscopy. Occasionally, it is necessary to place towels and blankets under the scapula, shoulders, nape of the neck, and head to flex the neck on the chest (see Figs. 17-1B and 17-2) and extend the head on the neck (see Figs. 17-1C and 17-2). In this instance, the purpose of the scapula, shoulder, and neck support is to give the head room so that it may be extended on the neck. When in doubt, the final assessment of the position should be from a lateral view of the patient, because only a lateral view enables precise assessment of the chest, neck, face, and head axes (see Figs. 17-1C and 17-2).
B Preoxygenation
Depending on the minute ventilation of the patient (spontaneous or assisted), the time to complete effective preoxygenation varies from 1 to 5 minutes; although in an awake and cooperative patient, this may be mostly accomplished with three or four full, vital capacity (VC) breaths.16,17 Work has documented the increased efficacy of eight full breaths in about 60 seconds, with times to desaturation approaching those of the more traditional 3- to 5-minute preoxygenation.18 A higher minute ventilation level leads to more rapid and complete preoxygenation. Measures of the adequacy of preoxygenation include real-time gas analysis of expired O2 concentration (goal = 95%) and analysis of expired N2 (goal < 5%). Essential to either of these measurements is the presence of a capnograph waveform with a plateau reflecting the expected alveolar carbon dioxide (CO2) concentration. This documents the presence of an effective seal of the circuit-bag system to the patient’s airway and the effective delivery of 100% O2. The use of an air-mask-bag unit (AMBU) without an expiratory valve may not provide optimal preoxygenation.19
The effectiveness of preoxygenation in preventing hypoxia during laryngoscopy is significantly reduced in the morbidly obese patient. Even with the most careful preoxygenation, the duration of apnea before the onset of hypoxia is one half of the duration seen in patients with normal body weight. This situation is attributed to the considerable reduction in FRC and VC in the obese patient and to the additional reduction attributable to the cephalad diaphragmatic shift related to supine positioning.20 This places morbidly obese patients at significantly increased risk for injury if any difficulty with ventilation or intubation is encountered.
Pharyngeal insufflation of O2 can significantly prolong the safe duration of apnea. In a typical adult, approximately 250 mL/min of O2 is transferred from the lungs into the bloodstream, while only 200 mL/min of CO2 enters the lungs from the bloodstream (respiratory quotient = 0.8). This alveolar gas deficit causes alveolar pressures to become slightly subatmospheric. If the airway is patent, there is a net flow of gas from the pharynx into the alveoli (apneic oxygenation). If, after adequate preoxygenation, the pharynx is filled with O2, the onset of hypoxia is delayed because O2, rather than air, is drawn into the lungs by this mechanism. Pharyngeal insufflation may be conveniently achieved by passing a catheter into the pharynx through a nasopharyngeal airway and attaching an O2 source at 2 to 3 L/min. Alternatively, some laryngoscopes have a side port suitable for attachment of O2 tubing. When preoxygenation is followed by pharyngeal insufflation as previously described, in normal but apneic patients, the O2 saturation from pulse oximetry [SpO2] remains equal to 98% for 10 or more minutes (although at the end of 10 minutes the arterial carbon dioxide tension [PaCO2] may be expected to be about 80 mm Hg).21
C Laryngoscopy
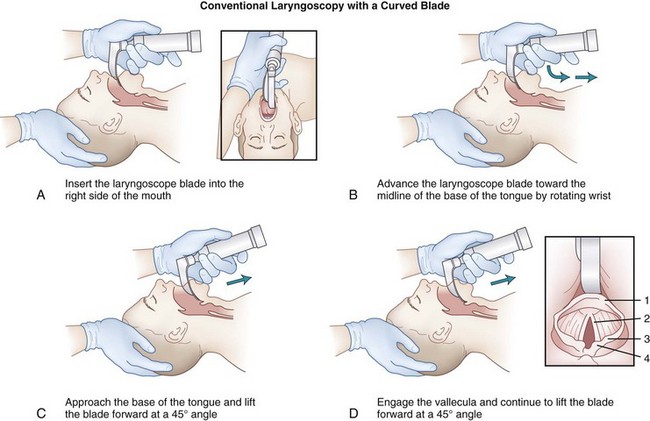
Two basic types of laryngoscope blades are the curved blade (Macintosh) and the straight blade with a curved tip (Miller).22,23 They are designed for right hand–dominant use; the laryngoscope is held in the left hand while the right hand manipulates the ETT. Historically, either hand (or both) could be initially used, shifting the laryngoscope to the left hand while the right hand manipulated the tube. Both blade styles include a flange on the left side of the blade for lateral retraction of the tongue and contain a light-emitting area (bulb or fiberoptic tip). Each blade has a channel with an open right side for visualization of the larynx and for insertion of the ETT (Figs. 17-3 to 17-10). Despite numerous modifications and variations, they are all lighted, handheld retractors for oropharyngeal soft tissues.
Related posts:
 Prehospital Airway Management
Prehospital Airway Management
 Medical-Legal Considerations: The ASA Closed Claims Project
Medical-Legal Considerations: The ASA Closed Claims Project
 Performance of Rigid Bronchoscopy
Performance of Rigid Bronchoscopy
 Nonintubation Management of the Airway: Airway Maneuvers and Mask Ventilation
Nonintubation Management of the Airway: Airway Maneuvers and Mask Ventilation

Full access? Get Clinical Tree


