Fig. 37.1
Setting and placement of the various equipment in the operating room. This setting is the same for all procedures of laparoscopic liver resection
Fig. 37.2
Trocar placement for laparoscopic partial hepatectomy
In our initial experience of laparoscopic partial hepatectomy, precoagulation by radiofrequency ablation was used before hepatic parenchymal dissection in laparoscopic wedge resection, primarily to minimize hemorrhage, to coagulate tissue surrounding the tumor, and to secure the surgical margin. The understanding obtained from the recent laparoscopic partial hepatectomies performed at our institution led to the following conclusions (Fig. 37.3a–c):
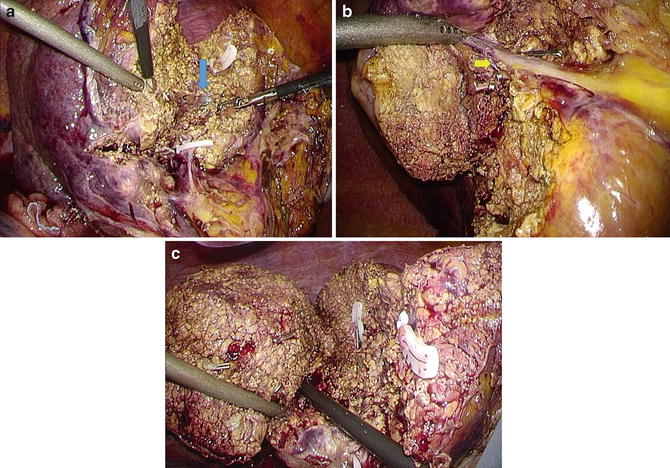
Fig. 37.3
(a–c) Laparoscopic partial hepatectomy. (a) To secure the surgical margin, perform the parenchymal dissection exposing the tributary of the middle hepatic vein (blue arrow). (b) Perform the partial hepatectomy of the segment XI along the posterior Glisson (yellow arrow). (c) Hanging up of the liver to prevent bleeding of the cut surface
An intermittent Pringle maneuver is necessary to minimize hemorrhage during hepatic parenchymal dissection.
In partial resection for HCC localized on the right lobe, mobilization of the right lobe by hanging it is necessary to control unexpected bleeding from the right hepatic vein.
To secure the surgical margin, the parenchymal dissection should be performed along the tributaries of the main hepatic vein or the tumor-feeding Glissonean pedicle, which form the landmark for the deep transection line.
Left Lateral Sectionectomy
The procedure is conducted by placing the supine patient in the reverse Trendelenburg position. Four ports are placed as shown in Fig. 37.4. CO2 pressure for pneumoperitoneum is kept at 8–10 mmHg during hepatic parenchymal transection. The round ligament and the falciform ligament are divided by a harmonic scalpel through the right port. The round ligament is grasped with Endoloop ligatures and pulled to the right using an Endo Close™ (Covidien, Dublin, Ireland) suturing device. The coronary ligament, the left triangular ligament, and the upper membrane of the hepatogastric ligament are divided with a harmonic scalpel to mobilize the left lateral section. The liver is then transected along the line near the left of the falciform ligament, using a harmonic scalpel. The liver parenchyma is transected to a depth of 2–3 cm by using a harmonic scalpel without the inflow occlusion to enable the insertion of an endoscopic linear stapler. Both portal pedicles, with the surrounding liver tissue, are divided using an Echelon Flex™ (Ethicon Endosurgery, Blue Ash, OH) stapler with a 60-mm gold cartridge. Thereafter, the left hepatic vein, including the liver parenchyma, is divided using the Echelon Flex™ stapler with a 60-mm white cartridge. Finally, the specimen is extracted using a protective bag through a suprapubic incision or a previous surgical incision. The technical requirements to safely and routinely perform laparoscopic LLS are as follows (Fig. 37.5a–c):
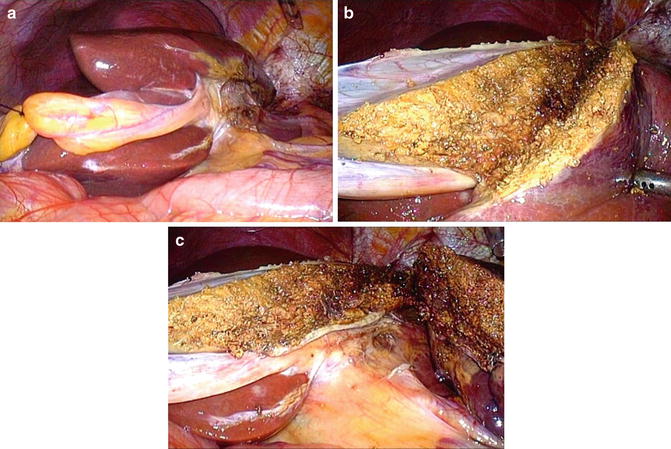
Fig. 37.4
Trocar placement for laparoscopic left lateral sectionectomy
Fig. 37.5
(a–c) Laparoscopic left lateral sectionectomy. (a) After dividing the surface of the hepatogastric ligament, mobilize the left lateral section enough to detect the Arantius duct. (b) Perform the parenchymal dissection, not exposing the portal pedicles of segments II and III. (c) Completion of dividing both portal pedicles with the surrounding liver tissue, using an Echelon Flex™ (Ethicon Endosurgery, Blue Ash, OH) stapler with a 60-mm gold cartridge
The surface of the hepatogastric ligament is divided with a harmonic scalpel to free the left lateral section.
In performing the liver parenchyma, neither the left hepatic nor the portal pedicles of segments II and III are exposed.
The branch form of the umbilical fissure vein [17] should be checked preoperatively.
Our procedure for pure LLS has been standardized and is reproducible. Hasegawa et al. reported that training new surgeons by allowing them to gain supervised experience with laparoscopic hepatectomy is both safe and feasible [18]. Further, they specified that LLS is a useful operation to train surgeons prior to more complex laparoscopic hepatectomy procedures [18]. Presently, there is a trend in favor of a pure laparoscopic approach for LLS for pediatric living donor liver transplantation, which can be considered as a safe procedure with potential advantages provided by the laparoscopic technique [19].
Major Hepatectomy
We have found a significant increase in the number of laparoscopic major hepatectomies performed over the past 2 years, with a concurrent reduction in the use of the hybrid method [20]. Initially, a laparoscopic trocar is inserted into the umbilicus using an open procedure and a 12-mm trocar is inserted under the xiphoid. Three further trocars are inserted in the subcostal region (Fig. 37.6), after which the supporting ligaments surrounding the resected side of the liver are resected and the liver is mobilized. Following cholecystectomy, the resected side of the hepatoduodenal ligament is skeletonized, and the right or left hepatic artery and the right or left portal vein are encircled with a piece of vessel tape, paying careful attention not to damage the branch for segment I and, if necessary, dividing it. Following division of the inflow vessels, the liver demarcation defines the transection line, marked on the liver surface with monopolar cautery, and intraoperative ultrasound is used to identify the middle hepatic vein, which is a deep resection line landmark. Once the parenchymal transection has begun over the hilar plate to detect the middle hepatic vein, it continues by keeping the cut plane between the middle hepatic vein and the demarcation line on the liver surface. The hepatic parenchymal transection is performed using the vessel-sealing device and clips, while a CO2 pneumoperitoneum is created and maintained at 12 mmHg. The specimen is externalized through a suprapubic incision in a section without muscle and placed in a large plastic bag. The incision is closed, the pneumoperitoneum reestablished, and hemostasis and biliostasis of the cut surface are checked. Finally, the drain is inserted near the cut surface from the trocar’s hole.
 End Points of Resuscitation
End Points of Resuscitation
 Cardiac Surgery Advances: Do We Still Remember How to Do the Open Bypass?
Cardiac Surgery Advances: Do We Still Remember How to Do the Open Bypass?
 The Role of Robotics in Selective Thoracic Surgical Problems: Technical Considerations
The Role of Robotics in Selective Thoracic Surgical Problems: Technical Considerations
 New Minimally Invasive Treatments for Acid Reflux
New Minimally Invasive Treatments for Acid Reflux
 Use of Biologic Grafts in Surgery
Use of Biologic Grafts in Surgery
 Brain Cancer: The New Frontiers
Brain Cancer: The New Frontiers



Related posts:
End Points of Resuscitation
Cardiac Surgery Advances: Do We Still Remember How to Do the Open Bypass?
The Role of Robotics in Selective Thoracic Surgical Problems: Technical Considerations
New Minimally Invasive Treatments for Acid Reflux
Use of Biologic Grafts in Surgery
Brain Cancer: The New Frontiers
Full access? Get Clinical Tree
