Fig. 30.1
Hand-assisted surgery setup with surgeon using nondominant hand in port and additional laparoscopic trocars using instruments and camera

Fig. 30.2
Intraoperative picture showing the use of the hand intra-abdominally to retract and allow for dissection
Hand-assisted surgery has been used in many different general surgical cases but is best suited for complex cases where removal of organs mandates a larger incision than the traditional laparoscopic port site. One particular general surgical arena where hand-assisted surgery is often used is in colorectal surgery. Laparoscopic colorectal surgery is a difficult laparoscopic case that often requires the removal of the colon with associated mesentery and lymph nodes. The extraction incision used by many surgeons is often several centimeters and, in some cases, the procedure can be performed more efficiently using the hand-assisted approach. Recent systematic reviews comparing the use of hand-assist and conventional laparoscopy for colorectal surgery showed decreased conversion rates with the use of hand-assisted surgery [2, 3] and no difference in outcomes [2]. These systemic reviews had mixed reports on operating times with one reporting decreased time with hand-assisted surgery [3] and the other showing no difference [2].
Microlaparoscopy/Needlescopic Surgery
After surgeons applied minimally invasive techniques to most commonly performed general surgical procedures, innovators in laparoscopic surgery began work to make the surgeries more minimally invasive. The initial enthusiasm involved single incision surgeries using special access cannulas and instruments that allowed abdominal entry through one incision. This enthusiasm in single incision surgery has rekindled the interest in microlaparoscopic and needlescopic techniques. Needlescopy employs the use of very small trocars and instruments no larger than 3 mm in diameter (Fig. 30.3).
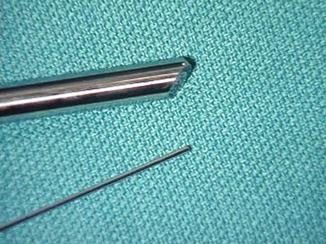
Fig. 30.3
Size comparison of traditional 10 mm laparoscopic versus the 3 mm laparoscope used in needlescopic surgery
The reasons surgeons began to experiment with needlescopy are the same reasons surgeons initially started using laparoscopes instead of open incisions; less tissue damage and less patient pain with better cosmesis and less fascial disruption, which potentially produces fewer hernias. Needlescopic instruments are smaller than traditional laparoscopic trocars and result in less tissue damage and thus potentially produce these beneficial patient endpoints.
Early studies in the surgical literature in the mid- to late 1990s initially assessed the feasibility of some basic laparoscopic procedures such as appendectomy, cholecystectomy, and diagnostic laparoscopy (Figs. 30.4 and 30.5). Other more complicated procedures were reviewed, such as Heller myotomy, splenectomy, cyst marsupialization, adrenalectomy, colon resection, sympathectomy, Nissen fundoplication, and inguinal herniorrhaphy.

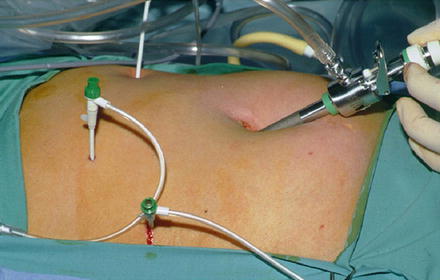
Fig. 30.4
Laparoscopic appendectomy utilizing two 3 mm needlescopic ports and an additional 5 mm port
Fig. 30.5
Laparoscopic cholecystectomy utilizing three 3 mm needlescopic ports and one 11 mm camera port
Larger studies emerged comparing needlescopy and laparoscopy with appendectomies and cholecystectomies. These are two of the most common laparoscopic procedures performed in America and are easily mastered by the general surgeon, making them good procedures to embark with a potentially technically challenging advancement. Naturally studies started out as retrospective comparisons and moved to small prospective studies and eventually larger controlled, randomized trials. Primary endpoints for early studies included operative time, technical feasibility, cosmesis, postoperative pain, complications, hospital stay, and conversion rates. As expected, the results of these studies were sometimes contradictory.
Two large systematic reviews comparing needlescopic and laparoscopic cholecystectomies showed that needlescopy is feasible and as safe as laparoscopy with similar hospital stays. Postoperative pain and cosmesis were improved with needlescopy in one study, while there was only a trend toward improvement in the other. Both studies found that conversion to open was higher in the needlescopy group. The results of a review comparing needlescopic and laparoscopic appendectomies mirrored those of the cholecystectomy reviews. Some of the results were in line with their expectations, such as the safety of the procedure, the longer operative times as the new technology is mastered, and improved cosmesis since the length of one or more incisions is reduced by nearly half [4, 5].
With smaller instruments and tissue damage, one would expect less postoperative pain, but only one of the reviews found less postoperative pain while the other did not, and the individual studies correspond to these findings [6–9]. One potential reason for the pain outcome is the use of some traditional sized trocars during needlescopic surgery, since the laparoscopic ports for the studied procedures were not entirely replaced with needlescopic instruments. Five millimeter ports are needed for modern laparoscopes as adequate optics for laparoscopes smaller than 5 mm are still being developed. Ten millimeter or even in some cases 12 mm ports are still required for specimen retrieval. These ports are also required for some advanced laparoscopic tools that are only available in 10 mm size, and surgical staplers require 12 mm ports as well. As a result of these unchanged port sizes, the patient’s pain is unlikely to change, as these larger port sites are the source of considerable postoperative pain. Similarly, the hospital stay is unchanged with patient pain remaining unchanged. Furthermore, the hospital stay for appendectomies and cholecystectomies is so short that any statistical diminution in that time would be difficult to show in studies.
Needlescopy is a safe alternative to traditional laparoscopy but still has limitations in many general surgery cases. Lack of sufficient technology to this point has limited significant conversion from normal laparoscopic trocars to needlescopic instruments. Advances in needlescopic technology continue and are focused on firmer instruments and adequate 3 mm camera optics. As we advance our knowledge and skill in laparoscopy, needlescopic advancements are sure to follow and may allow many general surgical procedures to employ 3 mm or smaller instruments and cameras that are as useful as the 5 and 10 mm instruments we use today.
Single Incision Surgery
Multiport laparoscopy has been the gold standard for minimally invasive surgery and has allowed surgeons to perform many complex laparoscopic surgeries using the cornerstone concepts of triangulation of ports. The ability to triangulate ports and access allowed surgeons to work ergonomically with good visualization of the target organ.
As was the case with the advent of laparoscopic surgery, the beginnings of the use of single incision surgery started with cholecystectomy. With the introduction of the possibility of removing gallbladders through the colon or vagina [10, 11], surgeons became more interested in more minimally invasive ways to remove gallbladders and noticed some of the shortcomings of the NOTES approach. Navarra had initially hypothesized the use of a single incision for cholecystectomy in 1997 [12], but this did not gain wide acceptance until approximately 10 years later. Since 2008, single incision surgery, which has been referred to as laparoendoscopic single site surgery (LESS), single port access (SPA), transumbilical endoscopic surgery (TUES), and single incision surgery (SILS), has gained modest popularity and use and been applied to most abdominal general surgical procedures.
Cholecystectomy has been the most common procedure performed using the single incision technique and has the most data supporting its use. Initial reports of single incision cholecystectomy showed feasibility and safety, and many different techniques have been described. Initially, techniques involved multiple trocars being placed at slightly extended umbilical incisions and use of conventional instrumentation. As technology improved, commercially available platforms for placement of three to four trocars became available as well as specially designed instruments and cameras that assisted with these procedures including flexible tip laparoscopes and curved instruments (Fig. 30.6). During early experience and with the learning curve of single incision surgery, additional trocars were sometimes required and recommended to aid in completion and achieve a safe laparoscopic surgery (Fig. 30.7). Some of the initial criticism and concern regarding using single incision techniques included the potential for more hernia formations with larger umbilical incisions, the potential for more bile duct injuries, and, for those performing the technique by placing sutures through the gallbladder for assistance in retraction, the possibility of spillage of tumor in unsuspected gallbladder cancer cases. Other concerns related to the thoroughness of the dissection and ability to obtain the critical view as well as the feasibility of performing cholangiograms, which were addressed by several authors [13–15].


Fig. 30.6
Single incision laparoscopic cholecystectomy utilizing a commercially available single incision port allowing four instruments to be placed. Flexible tip laparoscopes greatly aid in single incision surgery allowing better visualization and ergonomics
Fig. 30.7
Single incision laparoscopic cholecystectomy with ports placed within umbilical incision and additional 3 mm needlescopic port used for retraction
Since many different techniques were initially described for single incision laparoscopic cholecystectomy and since many surgeons found the technique to be challenging with a steep learning curve, a consensus statement was published in an attempt to standardize the technique based on high volume experienced surgeons who had mastered the learning curve. They recommended a 12 mm vertical incision through the existing anatomic scar of the umbilicus followed by insertion of a single 4-trocar port and the use of a 5 mm deflectable tip laparoscope [16]. Their proposed technique included placing the laparoscope at the 8 O’clock position, a bariatric length rigid grasper at the 4 O’clock position to grab the fundus, and a rigid bent grasper placed at the 2 O’clock position to grab the infundibulum, and at the 10 O’clock position a dissector of the surgeon’s choice placed as the working port [16]. This configuration, per their report, allows retraction of the gallbladder in the cephalad and lateral direction, provides triangulation, and facilitates dissection of the cystic artery and duct to allow for the critical view, which is the standard technique for a four-port cholecystectomy [16].
As the data for single incision laparoscopic cholecystectomy has matured from safety and feasibility to comparative studies with four-port cholecystectomy, some of the enthusiasm for this technique has tempered. In a randomized clinical trial and two meta-analyses, single incision cholecystectomy was reported to be safe but had only modest benefits of possible decreased postoperative vomiting and some improvement in cosmesis with no significant benefit of decreased pain, shorter length of stay, or decreased complication rate [17–19]. A recent Cochrane review evaluated nine trials with 855 total patients comparing 4-port and fewer than 4-port cholecystectomy. The review showed insufficient data and low quality evidence to show clinical benefit of reduced port cholecystectomy and recommended less than 4-port cholecystectomy surgeries be reserved for well-designed randomized clinical trials [20].
Robotic Surgery
As robotic surgery is covered in detail in another chapter, only a brief overview is presented here. Few areas of laparoscopic surgery generate more controversy and interest than surgical robotics. Although laparoscopic surgery has penetrated nearly every procedure in general surgery, there are still some limits associated with the techniques and technology that fail to make it universal. Limitations associated with current laparoscopic surgery include rigid/inflexible instruments that provide only finite movements, two-dimensional visualization, fatigue and poor ergonomics associated with some procedures, and amplification of tremors. Advances in surgical robotics have attempted to lessen some of these limitations allowing surgeons flexibility in instrument motions, 3-D vision, and the ability to perform surgeries in a comfortable position. Currently the da Vinci® Surgical System (Intuitive Surgical Inc; Sunnyvale CA) is the only available robotic system approved by the Food and Drug Administration (FDA). This system consists of a control console, a tower for the insufflator and video electronics, and the patient side cart (Fig. 30.8a–c).
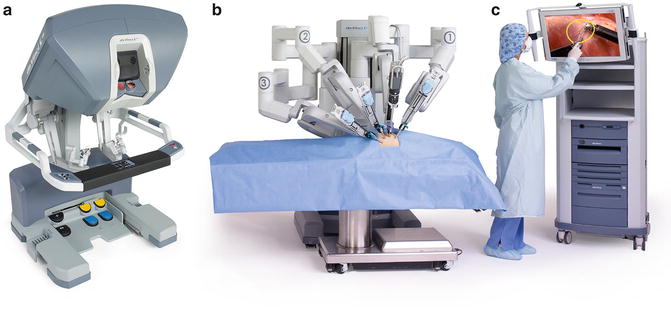
Fig. 30.8
(a–c) da Vinci® Si system (Intuitive Surgical Inc; Sunnyvale CA) with control console (a), the patient cart (b), and a tower for the insufflator and video electronics (c). (All: Used by permission. Copyright © 2015 Intuitive Surgical, Inc.)
Robotic surgery was initially adopted by urologists predominantly for the use in prostatectomy, but gynecologists were also early adopters of this technology. Only recently have general surgeons seen the potential value of robotic surgery. The slow adoption into general surgery is mostly related to the cases being performed by general surgeons and to some of the limitations of the current robot. The advantages of robotic surgery including improved visualization, the ability to work in confined spaces, and the need for complex motor tasks and suturing were sometimes outweighed by the limitations of the current surgical robot, which limits working in multiple abdominal quadrants, which is often needed for general surgical cases.
Related posts:
 End Points of Resuscitation
End Points of Resuscitation
 Cardiac Surgery Advances: Do We Still Remember How to Do the Open Bypass?
Cardiac Surgery Advances: Do We Still Remember How to Do the Open Bypass?
 The Role of Robotics in Selective Thoracic Surgical Problems: Technical Considerations
The Role of Robotics in Selective Thoracic Surgical Problems: Technical Considerations
 New Minimally Invasive Treatments for Acid Reflux
New Minimally Invasive Treatments for Acid Reflux
 Minimally Invasive Hepato-Pancreato-Biliary Surgery and Associated GI Interventions
Minimally Invasive Hepato-Pancreato-Biliary Surgery and Associated GI Interventions
 Brain Cancer: The New Frontiers
Brain Cancer: The New Frontiers

Full access? Get Clinical Tree


