Fig. 40.1
Incidence of osteoporotic disease
VCFs typically arise in an area with fewer bony trabeculae , which leads to a decrease in tensile strength, endplate compression, and finally a wedge compression deformity. Most often, VCFs are spontaneous, with little to no inciting event or trauma (see Fig. 40.2).
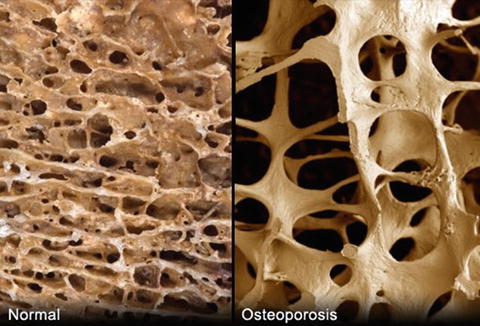
Fig. 40.2
VCFs typically arise in an area with fewer bony trabeculae , which leads finally to a wedge compression deformity
Approximately 85% of detected vertebral compression fractures cause moderate to severe pain. On average, the pain lasts for approximately 6–9 months, although many people have pain that lasts much longer. Not only do VCFs cause significant pain, but they also contribute towards a downward trend in daily activities and overall health (see Fig. 40.3). This has been called the vertebral compression fracture spiral. The downward spiral can include the following: pain leading to a reduction in ambulation, a reduction in exercise tolerance, a further decrease in bone density, additional compression fractures, a decrease in pulmonary function, rib crowding, decreased lung capacity, pneumonia, DVTs, other morbidities, and sometimes even death.
Fig. 40.3
VCFs contribute towards a downward trend in daily activities and overall health
Vertebral compression fractures are often undiagnosed. In many people, height loss from vertebral body fracture is very gradual and is often under-recognized until one has a high enough level of clinical suspicion to obtain a MRI (Fig. 40.4). Plain film X-rays are often initially ordered to evaluate new onset spinal pain. Unfortunately, X-rays do not always show a clear demarcation between fracture and non-fracture. Older chronic fractures often look the same as acute or subacute fractures; mild compression deformities are often not seen at all. One must remember that osteoporosis is a generalized disease and often affects other vertebral bodies, as well as other bones. If someone has one vertebral compression fracture, they may have another, and are certainly more susceptible to having future fractures as well.

Fig. 40.4
Height loss from vertebral body fracture may be very gradual and is often under-recognized until one has a high enough level of clinical suspicion to obtain a MRI
Osteoporotic vertebral compression fractures (VCFs) have become an increasingly important disease, not only due to their significant socioeconomic impact, but also due to the increasing age of our population [1]. Approximately 4% of patients presenting in the primary care setting with low back pain have a vertebral compression fracture [2, 3]. The painful progressive collapse of the vertebra and subsequent loss of posture are associated with a series of clinical consequences leading to an increased morbidity and mortality rate [4]. Many patients heal with conservative treatment, which consists of rest or activity modification, analgesics, and bracing. However, persistent severe pain compels some patients to seek a minimally invasive intervention via one of two procedures: vertebroplasty or kyphoplasty [1].
Vertebroplasty (VP) and kyphoplasty (KP) are minimally invasive percutaneous procedures, whereby an interventionist injects polymethylmethacrylate (PMMA) into fractured osteoporotic vertebral bodies, with the aim of immediate stabilization and pain relief [4]. PMMA, also known as “bone cement ,” is injected at low viscosity directly into the cancellous bone in the VP technique [4]. Kyphoplasty differs from VP through its inherent mechanism; KP is performed by inserting a hollow needle consisting of a contrast-filled inflatable balloon into the vertebral body, which is then carefully inflated to create a hollow space within the fracture (Fig. 40.5). This method allows a degree of fracture and pressure reduction, while leaving a cavity that is immediately filled with high-viscosity PMMA [4]. Both procedures provide a treatment for VCFs and exhibit a significant postoperative decrease in pain, as well as an increase in function [5–8].
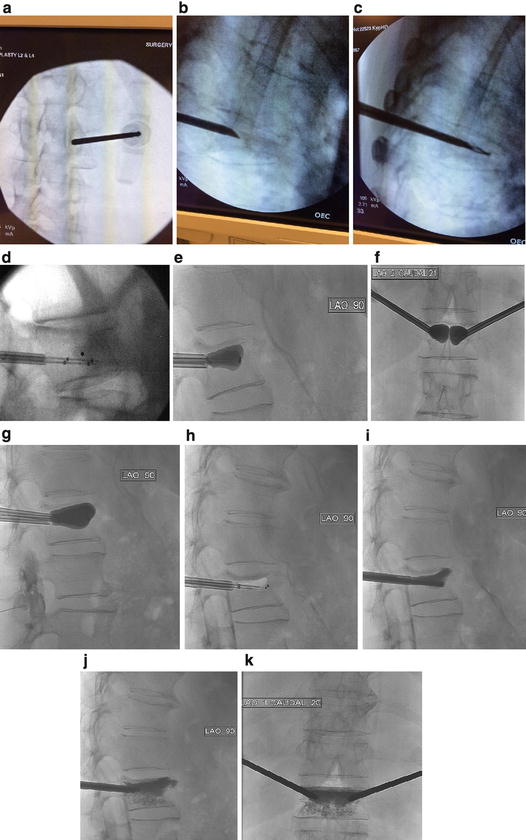
Fig. 40.5
Image sequence of kyphoplasty (KP) for vertebral fracture repair. Images courtesy of Arizona Pain and Wayne Olan, M.D. (a) Align the tip of the needle with the lateral and superior aspect of the pedicle. Verify on a lateral image that the tip is placed on the posterior wall of the pedicle and verify the trajectory of the needle. (b) When the needle tip arrives at the medial border of pedicle, verify entrance to the vertebral body on a lateral view. Advance the needle to approximately 4 mm past the posterior cortical wall. (c) Drill channels for balloons. (d) Insert balloons. (e, f) Inflate the balloon. (g) Maximum balloon distention is safely achieved. (h) Balloon deflation. (i) Deliver the cement. (j) Fill the cavities and then interdigitate. (k) In terms of cement volume, the trend is towards smaller volumes, but the volume delivered depends on the level treated (less for high thoracic and more for low lumbar), the caliber of vertebral body, and clinical goals. Typical volumes range from 1 to 4 cc
Background
The first percutaneous vertebroplasty was performed in France by Dr. Deramond in 1984 to fill a painful cervical hemangioma. Other physicians around the world later adopted this technique to treat VCFs. Revisions to the procedures helped physicians in the United States to address growing concerns of VCFs. While VCFs affect approximately 25% of postmenopausal women, the prevalence increases to 40% for women aged 80 and older [5, 9–11]. However, decreased bone mass , which is often seen in postmenopausal women, is not the only cause of VCFs. VCFs can also arise from metastatic cancer and trauma. Consequently, VCFs can cause the spine to progressively become weaker, rendering it unable to bear body weight. This sequence of events may lead to poor mobility, weight gain, depression, and a host of other side effects. Moderate to severe back pain subsequently develops, and a progressive loss of height may ensue.
Pathophysiology
Acute vertebral compression fractures occur when the weight of the upper body exceeds the ability of the bone within the vertebral body to support the load. Progressive reduction in trabecular bone mass from osteoporosis or inflammatory mediators creates porous bone, which subsequently increases the risk of fracture [12]. Poor diet, decreased estrogen (menopause), and lack of weight-bearing exercises can increase yearly bone loss, resulting in progression to osteoporosis. Patients with severe osteoporosis may experience a VCF from activities of daily living (ADLs) and from minor movements, such as stepping out of a vehicle, vigorous sneezing, or lifting light objects [13]. A healthy spine can sustain a compression fracture from severe trauma, such as an automobile accident, sports injury, or hard fall.
After sustaining an injury, the applied force usually causes the anterior portion of the vertebral body to crush, forming what is known as a “wedge fracture ” (Fig. 40.6) [9]. The middle column usually remains intact and can act as a hinge. Loss of anterior height of the vertebra ensues while the posterior height usually remains unaffected. As the collapsed anterior vertebrae fuse together, the spine bends forward, causing a kyphotic deformity [9]. Since the extent of damage is localized to the anterior vertebrae, the fracture is usually stable and is rarely associated with neurologic complications. A “burst fracture ” is considered when the entire vertebral body collapses (Fig. 40.7).
Fig. 40.6
“Wedge fracture ”
Fig. 40.7
“Burst fracture ”
Other causes of VCFs included malignancies, long-term corticosteroid use, trauma, and adolescents suffering from chronic rheumatologic disorders. Malignancies such as multiple myeloma can cause high serum levels of IL-6, which stimulates plasma cell growth and production of osteoclasts that in turn lead to vertebral body destruction [12]. Adolescents suffering from chronic ankylosing spondylitis (AS) for 20 years or more are prone to vertebral compression fractures due to rigidity and decreased bone mineral density [14]. Chronic AS releases inflammatory mediators, such as TNF-α and IL-6, which activate osteoclasts that may lead to osteopenia/osteoporosis; thereby, this increases fracture risk [14]. Long-term corticosteroid usage inhibits bone formation by altering osteoblast activity while causing osteocytes to undergo apoptosis, reducing bone formation, and inhibiting development of the cytoskeleton [15, 16]. Although the most common cause of vertebral compression fractures is osteoporosis [1], osteoporotic fractures are not the only cause of VCFs. It is incumbent to include VCFs as part of the differential diagnosis when a patient presents with back pain .
Diagnosis
Vertebral compression fractures cause characteristic signs and symptoms that may be revealed upon careful history and physical examination. In particular, patients usually present with constant and focal pain, which appears to be axial or non-radiating. Thoracic spine pain may transfer to the ribs and the patient may demonstrate some difficulty with large inspiratory and expiratory movements. The pain may also radiate to the abdomen, but this is less common. Upon physical examination, direct percussion or palpation along the spinous process of the affected level may reproduce or worsen the patient’s pain. Some also use a tuning fork over the affected spinous processes to see if the patient has concordant pain. In addition, careful history may reveal that the patient has pain that is worse while standing, sitting, and driving in a car. Pain may be partially relieved while lying down flat. Symptoms that radiate to the upper or lower extremities are likely due to another pathology.
Vertebral compression fractions are most commonly located in the mid-thoracic region from T6-T9, as well as the thoracolumbar junction from T11-L1. In the mid-thoracic region, spinal thoracic kyphosis is the most pronounced, which induces loading stress during flexion, making these vertebral body levels more susceptible to fracturing. In the thoracolumbar junction, the more rigid thoracic spine gives way to the mobile lumbar region, which makes these vertebral bodies more susceptible to fracture as well.
In the USA, 1.5 million vertebral compression fractures occur each year [17]. Only a third of these fractures are diagnosed [18, 19]. Patients typically present with acute back pain after sudden sneezing, coughing, stretching, lifting, or after minor trauma [13]. Even something as seemingly benign as riding over a speed bump can precipitate a fracture [20]. Palpation or percussion of the midline spine often reveals tenderness that may refer to the paravertebral musculature, flank, or abdomen. Often presenting without pain, height loss of >6 cm can be very specific (94%) for VCFs [21]. When using baseline height as a comparison, a 20% decrease of vertebral height or decrease of at least 4 mm identified on radiographs may be considered as a positive finding for a VCF [22]. Fractures may occur anywhere along the occiput to the sacrum, and careful imaging of the entire spine should be taken.
Plain frontal and lateral radiographs of the thoracolumbar spine can diagnose fractures through the lumbo-dorsal junction, mainly T8-T12, L1, and L4 [23]. Though radiographic imaging can reveal a fracture, magnetic resonance imaging (MRI) using the short tau inversion recovery (STIR) sequence is the gold standard for VCF assessment. MRI allows the documentation of the number of fractures. The STIR sequence is preferred for determining the age of a fracture (see Fig. 40.8). Specifically, presence of a fat signal surrounding a fracture indicates an older VCF that has healed. The presence of vertebral body marrow edema, bright white on T2 STIR sequencing, indicates an acute or subacute fracture that is unhealed. MRI can also reveal the extent of spinal canal encroachment and can be used to identify or to rule out other possible pain generators or malignancies.
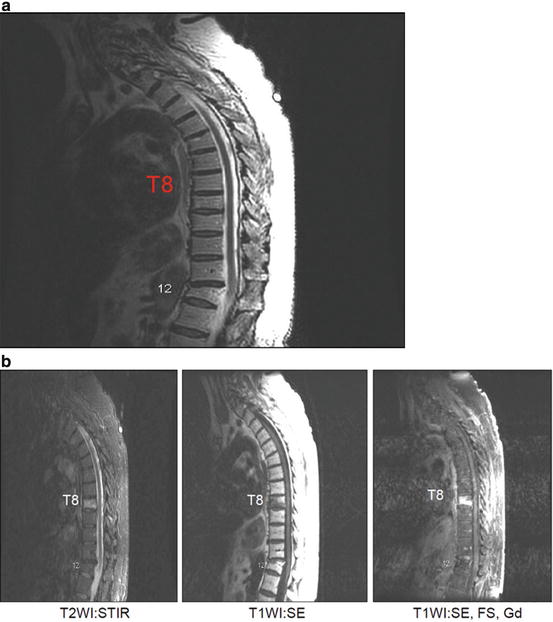
Fig. 40.8
Magnetic resonance imaging of a patient with fractures of the T8 and T12 vertebrae. Images courtesy of Wayne Olan, M.D. (a) MRI T2 images show T8 and T12 fractures. Acute and subacute fractures are not differentiated. (b) MRI STIR sequence images reveal an acute T8 fracture and chronic, healed T12 fracture.
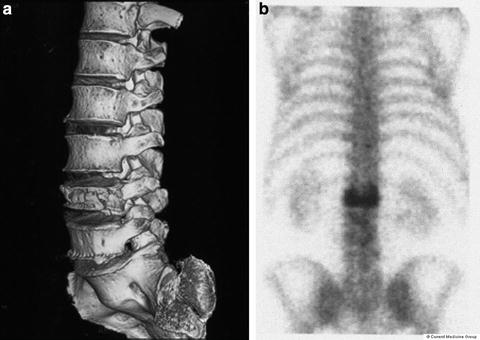
If one is unable to obtain a MRI (e.g., patient with cardiac pacemaker, spinal cord stimulator device), a combination of CT and bone scans are typically performed to diagnose and to classify the acuity of VCFs (see Fig. 40.9). On bone scans, bone uptake is markedly increased in acute fractures. It may be near normal in older, healed fractures. Caution is needed in interpreting bone turnover, as bone turnover tends to be low in older adult patients. Computerized tomography (CT) imaging, using sagittal and 3D reconstruction (if available), can be useful in such patients.
 Pain in the Stroke Rehabilitation Patient
Pain in the Neuromuscular Disease Rehabilitation Patient
Basic Psychopharmacology for the Treatment of Pain in the Rehabilitation Patient
Intrathecal Therapy for the Treatment of Pain in the Rehabilitation Patient
Pain in the Stroke Rehabilitation Patient
Pain in the Neuromuscular Disease Rehabilitation Patient
Basic Psychopharmacology for the Treatment of Pain in the Rehabilitation Patient
Intrathecal Therapy for the Treatment of Pain in the Rehabilitation Patient
 Intra-articular Joint and Bursa Injections for the Treatment of Pain in the Rehabilitation Patient
Intra-articular Joint and Bursa Injections for the Treatment of Pain in the Rehabilitation Patient
 Chiropractic Medicine for the Treatment of Pain in the Rehabilitation Patient
Chiropractic Medicine for the Treatment of Pain in the Rehabilitation Patient



Related posts:
Pain in the Stroke Rehabilitation Patient
Pain in the Neuromuscular Disease Rehabilitation Patient
Basic Psychopharmacology for the Treatment of Pain in the Rehabilitation Patient
Intrathecal Therapy for the Treatment of Pain in the Rehabilitation Patient
Intra-articular Joint and Bursa Injections for the Treatment of Pain in the Rehabilitation Patient
Chiropractic Medicine for the Treatment of Pain in the Rehabilitation Patient
Full access? Get Clinical Tree
