1. Pancreas preservation method and solution:
a. Cold storage: UW solution, HTK solution, ET-Kyoto solution
b. The two-layer method: UW/oxygenated PFC, ET-Kyoto/oxygenated PFC
c. Ductal preservation: ET-Kyoto solution
2. Clinically used collagenase for distention and Ricordi method:
a. Liberase MTF, Serva Nb1, CIzyme
3. Islet purification method:
a. Continuous density gradient using COBE 2991 cell processor
b. Continuous density gradient using large bottle method
Pancreatic ductal preservation could improve the success rate of clinical islet isolation [13]. The pancreatic ductal preservation is performed immediately after pancreas procurement. The ET-Kyoto solution (approximately 1 ml/g pancreas) is directly injected into the main pancreatic duct. This method improved distribution of collagenase at the time of pancreas distention with collagenase [14].
Islet Isolation Technology
The islet isolation technology consists of pancreas distention with collagenase solution, pancreas digestion, and islet purification (Table 42.1, Fig. 42.1a–c). Selection of collagenase is one of the important factors for successful islet isolation. Previously, Liberase HI (Roche, Basel, Switzerland) was widely used. However, due to safety issues, it is no longer used. New Liberase MTF (Roche), CIzymeTM (Viacyte, San Diego, CA), and NB1 (Serva Electrophoresis, Heidelberg, Germany) are currently used.
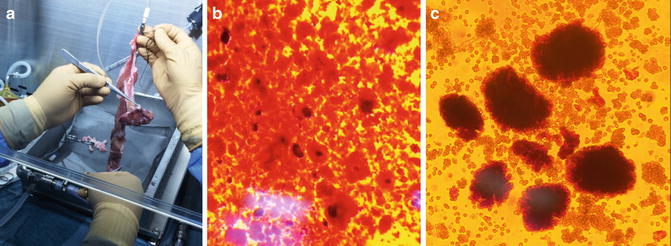
Fig. 42.1
Porcine islet isolation process. (a) Distended pancreas with collagenase solution. (b) Digested pancreas using Ricordi method. (c) Purified islets after the bottle purification method
The Ricordi method has been widely used for pancreas digestion [15]. Distended pancreas is cut into 7–10 pieces and put into Ricordi chamber. During the digestion phase, collagenase solution is recirculated in the close-loop system connected to Ricordi chamber. Once pancreas is digested and free islets are released, the digested pancreas is collected in the massive amount of dilution solution using peristaltic pump at a rate of 300 ml/min. This immediate and massive dilution can prevent over-digestion of isolated islets.
Islets are purified from the digested pancreas using the density gradient and centrifugation method. A continuous density gradient with Ficoll® (VWR, Radnor, PA) solution or iodixanol solution in the COBE® 2991 cell processor (Terumo BCT, Lakewood, CO) is widely used. Recently, it was demonstrated that a continuous density gradient in a large bottle and centrifugation provided better islet yield [16]. The large bottle method is a simple method and avoids using an expensive COBE 2991 cell processor.
New Immunosuppression Protocol
The Edmonton protocol introduced a glucocorticoid-free immunosuppression regimen. Daclizumab is used for induction and tacrolimus and sirolimus are used for maintenance [2]. T cell depletion immunosuppression protocol substantially improved long-term islet function, and several groups achieved up to 50 % insulin independence beyond 5 years after islet transplantation, which is comparable to the pancreas alone transplantation [5].
Achieving insulin independence with single donor is another important target for islet transplantation to ameliorate the donor shortage. See Table 42.2. Hering et al. demonstrated that careful donor and recipient selection and T cell depletion using thymoglobulin or OKT-ala-ala antibody enabled them to achieve single-donor islet transplantation [17]. The Illinois group demonstrated that exenatide enables them to achieve insulin independence with single donor. Exenatide is a GLP1 analog which has several advantages for islet transplantation including enhancing of insulin-secretary ability, beta-cell proliferation, and loss of appetite. The San Francisco group introduced new immune suppression drugs, Efalizumab and Belatacept, which enables them to achieve insulin independence with single donor. Both Efalizumab and Belatacept are co-stimulatory blockage: Efalizumab blocks anti-LFA-1 and Belatacept blocks CD80-CD86 pathways. Finally, T cell depletion and potent anti-inflammation using the double blockade with IL-1 beta and TNF alpha enabled us to achieve insulin independence with single-donor islet transplantation [11]. Notably, this protocol did not use sirolimus which has notorious side effects including oral ulcer, peripheral edema, hyper lipidemia, and so on.
Table 42.2
Published successful single-donor islet transplantation
Center | Year | Induction | Maintenance | Donor | Insulin free |
|---|---|---|---|---|---|
Minnesota | 2004 | Anti-CD3 | Sirolimus, Tacrolimus | Single donor | 4/6 |
Minnesota | 2005 | ATC, Daclizumab, Etanercept | MMF, Sirolimus, Tacrolimus | Single donor | 8/8 |
Miami | 2005 | Daclizumab | Sirolimus, Tacrolimus | 1 or 2 donors | 7/8 |
Miami | 2005 | Daclizumab, Infliximab | Sirolimus, Tacrolimus | 1 or 2 donors | 7/8 |
Kyoto | 2005 | Daclizumab | Sirolimus, Tacrolimus | Single living donor | 1/1 |
Illinois | 2008 | Daclizumab, Etanercept, Exenatide | Sirolimus, Tacrolimus | Single donor | 6/6 |
San Francisco | 2010 | ATG | Efalizumab, Sirolimus or MMF | 1 or 2 donors | 4/5 |
San Francisco | 2010 | ATG | Belatacept or Efalizumab, and Sirolimus or MMF | Single donor | 3/5 |
Baylor | 2011 | ATG, Etanercept, Anakinra | Tacrolimus, MMF | Single donor | 3/3 |
Next Target of Islet Cell Transplantation
Even though allogeneic islet transplantation continuously improves the clinical outcomes, this therapy never cures majority of type 1 diabetic patients due to insufficient donors. Insulin-producing cells from nonhuman donor are required to fulfill the goal. The possible nonhuman donor sources are xenografts, embryonic stem (ES) cells, and induced pluripotent stem (iPS) cells. Among the cells, xenografts derived from porcine pancreas have been clinically used since 1994 [18]. However, possible infection with porcine endogenous retrovirus (PERV) after islet xenotransplantation in SCID mice was reported, and PERV became the major concern for the porcine islet transplantation [19]. Furthermore, International Xenotransplantation Association published their statement that only a well-coordinated international effort aimed at harmonizing xenotransplantation procedures according to the highest ethical and regulatory standards on a global scale will enable the initiation of clinical xenotransplantation trials under the best auspices for its success and minimizing risk of failure [20]. In New Zealand, encapsulated neonatal porcine islet transplantation has been conducted under the comprehensive regulatory framework for the first time [21]. Thus, the islet transplantations using porcine xeno islets are already a clinical reality. Of note, porcine islet transplantation has several advantages over allogeneic transplantation besides solving donor shortage, such as well-characterized donor, scheduled procedure, and possible gene modification (Table 42.3).
Table 42.3



Advantages and disadvantages of porcine islet over allogeneic islet
Related posts:






Full access? Get Clinical Tree
