(1)
Chennai Breast Centre, Chennai, India
Invasive carcinoma (NOS) type is the most common invasive breast carcinoma, accounting for up to 80 % of all invasive breast cancer. All invasive cancers that cannot be called a specific type like lobular, tubular, medullary, mucinous, or papillary cancers are grouped together in one category as NOS – not otherwise specified. Hence, they are a heterogeneous group of lesions with varying clinical, imaging, and histological features.
Clinical Features
They may be nonpalpable lesions if diagnosed with screening mammography (Fig. 31.1).
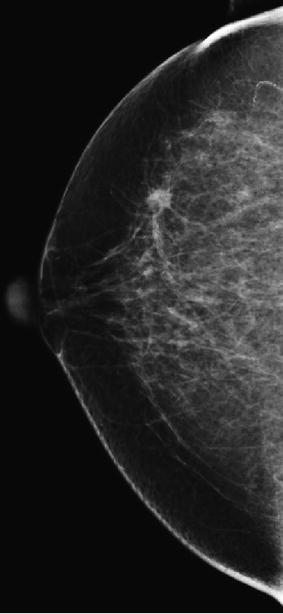
Fig. 31.1
Screen-detected nonpalpable malignancy
Symptomatic patients may present with a mass, pain, or nipple discharge. Large masses may involve the skin, producing peu de orange appearance, skin retraction, nipple retraction, and metastatic axillary lymph nodal enlargement.
Mammographic Findings
The mammographic appearances of invasive ductal carcinoma–NOS are very variable. They commonly present as spiculated, indistinct, or sometimes circumscribed masses (Figs. 31.2a–c and 31.3a–c). There may be architectural distortions and associated findings like skin thickening, skin tethering (Fig. 31.4), Nipple areolar complex thickening, nipple retraction, and axillary nodal enlargement (Figs. 31.5a, b and 31.6a, b) Over 50 % of masses will be associated with calcifications. Multifocal tumors and multicentric tumors are present in over 20–30 % of invasive duct carcinomas (Fig. 31.7a, b). Multifocal tumors are described as tumors within the same quadrant and multicentric tumors are defined as tumors occurring in different quadrants of the breast (Figs. 31.8a–c and 31.9a–c).
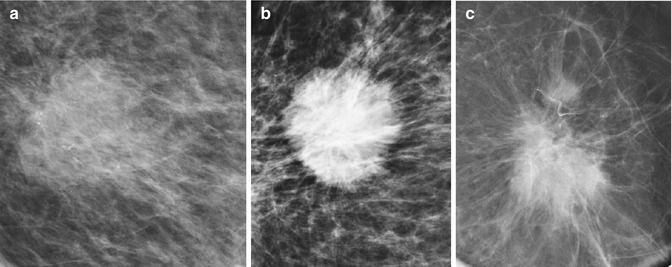
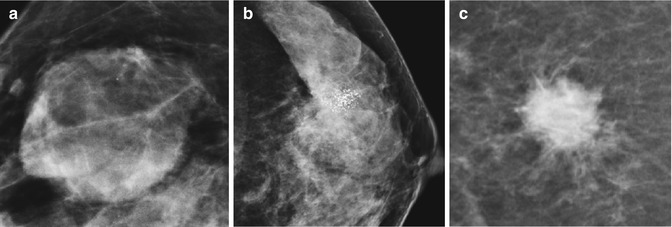
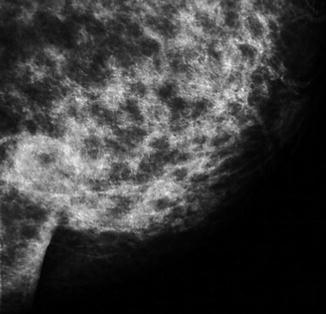
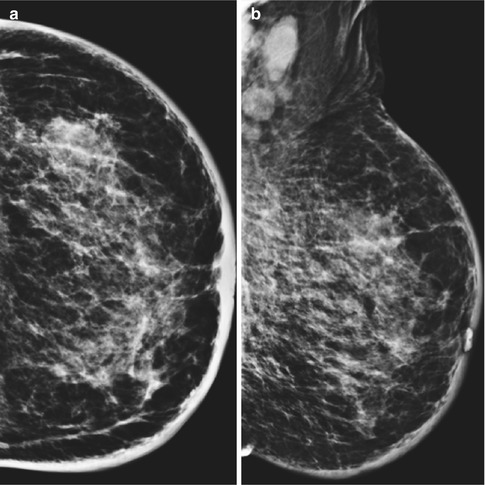
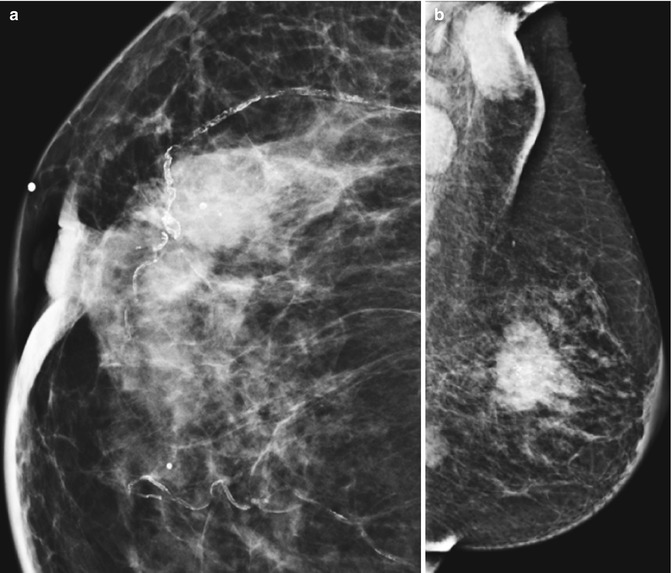
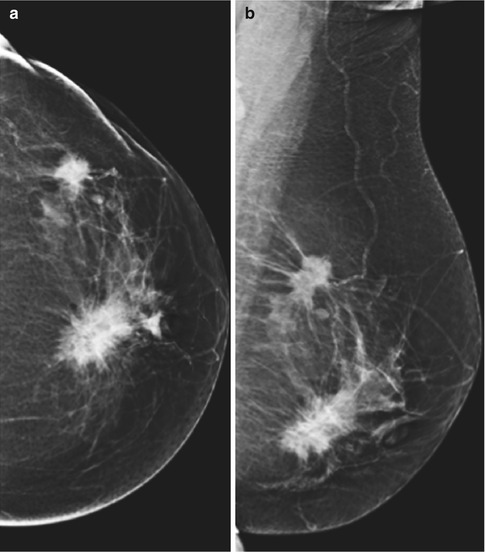
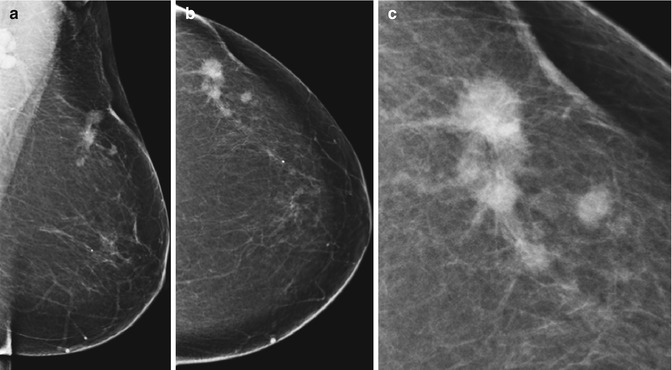
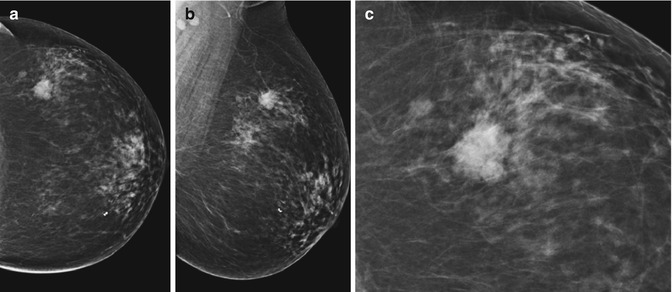
Fig. 31.2
Heterogeneity in breast cancer. (a) Malignant lesion on a mammogram with indistinct margins, (b) microlobulated mass, and (c) spiculated lesion
Fig. 31.3
(a–c) A well-circumscribed lesion. HPE: high-grade, triple-negative malignancy. (b) Indistinct mass with calcifications and architectural distortion producing a tent sign. (c) Circular lesion with partially indistinct margins. HPE: mucinous carcinoma
Fig. 31.4
Malignant mass with architectural distortion producing an angle (elbow sign)
Fig. 31.5
(a, b) CC and MLO mass lesion with skin thickening, trabecular thickening, and axillary lymph node enlargement
Fig. 31.6
(a) Malignant mass lesion with nipple areolar thickening and retraction. (b) MLO view showing multicentric malignancy with axillary lymph node enlargement, skin retraction, and nipple areolar thickening
Fig. 31.7
(a, b) CC and MLO views showing multicentric malignancy
Fig. 31.8
(a–c) CC, MLO, and optically magnified images showing multifocal malignancy, with skin thickening and retraction
Fig. 31.9
(a–c) CC, MLO, and optically magnified images showing multifocal breast cancer
Spiculated Cancers
Spiculated cancers are paucicellular and likely to be lower grade tumors. The tumor incites an intense desmoplastic reaction that produces the spiculations. The intense fibrous stromal reaction produces a hard palpable mass that gives the name “schirrous” cancer.
Circumscribed Cancers
Most circumscribed invasive cancers are specified types like medullary or mucinous types, but a small percentage of NOS type presents with circumscribed lesions. These are usually very high grade and cellular and often triple negative (ER, PR, and Her 2 negative). Even circumscribed cancers may have partially obscured, indistinct, or microlobulated margins in a small portion of the tumor margins.
Architectural distortion may be seen as converging lines, straight lines, bulging lines, tenting and elbowing along the gland fat interface in the premammary and retromammary zone may be signs of an invasive ductal cancer.
Calcifications are seen in over 75 % of invasive breast cancer NOS. The calcifications may extend well beyond the mass either towards the nipple or away from the nipple. The extent of the calcifications beyond the lesion determines the nature of breast surgery, i.e., breast-conserving surgery or a mastectomy.
Related posts:






Full access? Get Clinical Tree


