Figure 13.1. Technique for intravenous regional anesthesia. A small intravenous catheter is placed in the hand and the tourniquet is applied to the upper arm. A single tourniquet may be used for shorter operations and may provide more reliable compression of the venous system than the double-tourniquet system shown. Exsanguination of the arm is attained by elevation and wrapping with the Esmarch elastic bandage. The tourniquet is then inflated and the local anesthetic injected.
b. If the procedure exceeds 45 minutes, the double cuff may be employed. In this situation, the proximal cuff is inflated for the first 45 minutes of anesthesia. The distal cuff is then inflated over the tissue area that has been numbed by the local anesthetic injection and the proximal cuff (overlying unanesthetized skin) is deflated. The adequacy of the distal cuff must be checked before the proximal cuff is deflated. Although this technique allegedly reduces patient discomfort at the area of the tourniquet, the complex procedure of shifting the inflation adds the risk of unintentional deflation.
4. Injection of local anesthetic solution
a. After exsanguination, the limb is returned to the neutral position and the local anesthetic drug is injected through the previously placed catheter. The injection is made slowly (90 seconds or more) to produce a peak venous pressure that is not greater than the occluding pressure of the cuff (13).
b. The patient is warned that this will produce an uncomfortable “pins and needles” sensation for a few seconds. Slow rate of injection may reduce this discomfort.
c. The catheter is removed if surgery will be less than an hour, and pressure is placed over the entry site until it seals. Adequate sensory anesthesia will ensue in 5 minutes.
d. If more than 45 minutes have elapsed from the time of injection, anesthesia may begin to diminish. If the surgeon requires more time, the intravenous catheter may be reinjected with local anesthetic solution after 60 to 90 minutes. This is disruptive to the surgery and potentially to the sterile field, and, because of this, for longer procedures, other regional techniques, such as brachial plexus block, are usually a more appropriate plan.
5. Cuff deflation
a. Deflation of the tourniquet can be performed after 45 minutes with minimal risk of systemic symptoms of local anesthetic toxicity because the drug binds to the tissues (14).
b. If less than 45 minutes have elapsed, a two-stage release is recommended, where the cuff is deflated for 10 seconds and reinflated for a minute before final release. This allows a gradual washout of anesthetic. Cycling the cuff three times in this manner will delay the onset of peak blood levels, but it does not significantly reduce the level attained with a single deflation (15).
c. Under no circumstances is the cuff deflated in the first 20 minutes after injection. If less than 20 minutes have elapsed, pleasant conversation should be used to fill the time until that interval has passed and a two-stage release can be performed. These steps do not guarantee the absence of systemic toxicity (Figure 13.2).
V. Complications
A. Systemic toxicity is the major risk of this procedure.
1. The greatest danger is from an inadequate tourniquet early in the procedure when the intravenous volume and concentration are large. Every precaution must be taken to ensure a reliable tourniquet and inflation pressure source.
2. Even with adequate inflation, the narrow cuffs (5–7 cm width) used for the double-tourniquet system will sometimes allow leakage. The use of a standard width adult cuff (12–14 cm) provides more reliable compression of the entire venous system of the extremity, especially in the leg.
3. Leakage is more likely if the injection is made rapidly under high pressure into a vein near the cuff (13).
4. The least leakage occurs when injection is made into a distal vein for more than 90 seconds following exsanguination of the arm and inflation of the cuff to 300 mm Hg pressure. Careful monitoring of mental status is indicated for several minutes, even with an apparently functioning cuff.
5. Tourniquet release inevitably washes drug into the systemic circulation as some local anesthetic remains in the veins at the end of the procedure. With lidocaine, these levels are subtoxic after 45 minutes, but dangerously high within 20 minutes of injection (14). This is the basis for the guidelines for tourniquet release stated.
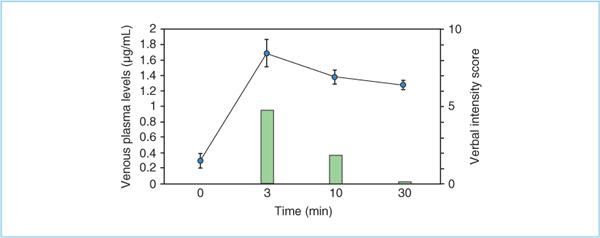
Figure 13.2. Systemic blood levels of 0.5% lidocaine after intravenous regional blockade. After release of the tourniquet, blood levels of local anesthetic increase rapidly, but are also rapidly cleared. After 72 ± 22 minutes of total tourniquet inflation time, the colored circles indicate blood levels following injection of 40 mL of 0.5% lidocaine (range to 2 μg/mL). The solid bars indicate the verbal numerical intensity score (on scale of 0–10) of central nervous system symptoms of light-headedness, dizziness, and tinnitus at 3, 10, and 30 minutes after deflation. (Adapted from Atanassoff PG, Hartmannsgruber MWB. Central nervous system side effects are less important after iv regional anesthesia with ropivacaine 0.2% compared to lidocaine 0.5% in volunteers. Can J Anaesth 2002;49:169–172.)







Full access? Get Clinical Tree


