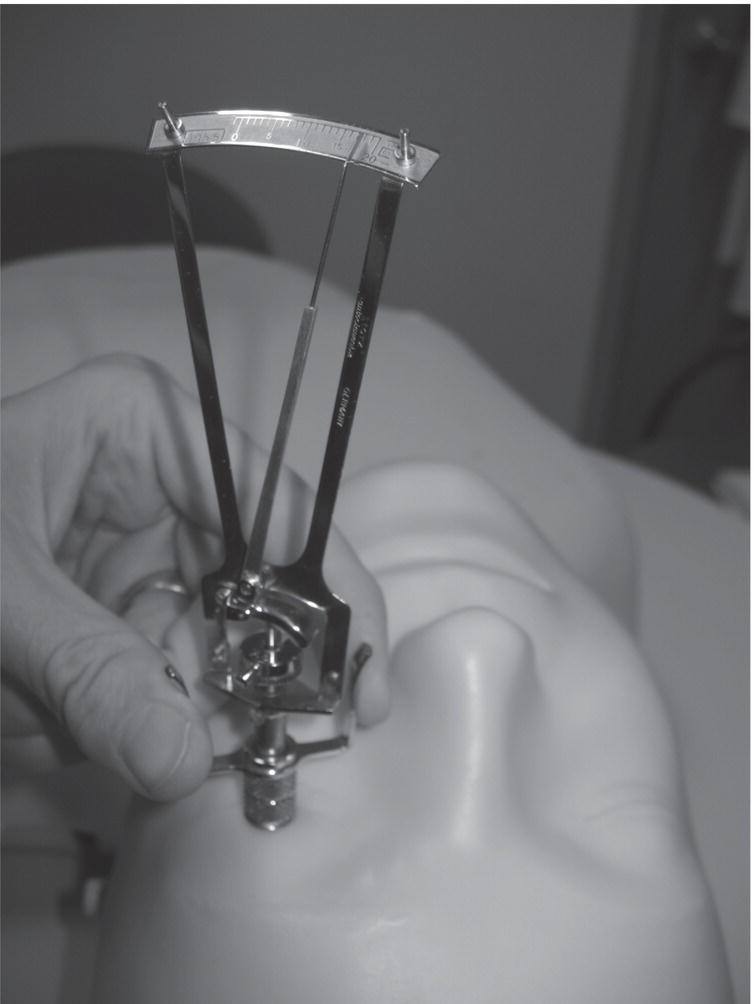
Ali S. Raja1 and Jesse M. Pines2,3 1 Department of Emergency Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA 2 US Acute Care Solutions, Canton, OH, USA 3 Department of Emergency Medicine, Drexel University, Philadelphia, PA, USA Glaucoma is a leading cause of blindness and visual impairment worldwide and occurs as a result of increased intraocular pressure (IOP), which is typically due to either acute narrowing of the anterior chamber angle (angle closure glaucoma) or progressively decreasing aqueous humor outflow and increasing aqueous humor production (open‐angle glaucoma). Patients may seek acute care for symptoms related to elevated IOP that include not only eye pain but also visual impairment, nausea, vomiting, and headache. Measuring IOP is an essential component of the evaluation of patients suspected of having glaucoma (of both the acute closed‐angle and open‐angle types) as well as blunt eye trauma and iritis. Measurements above 20–22 mmHg are abnormal and should prompt evaluation by an ophthalmologist, either in the acute care setting or through urgent referral. Figure 53.1 The Tono‐Pen XL tonometer. Different methods of measuring IOP are available and are broadly divided into applanation, indentation, noncontact (air puff), rebound, and transpalpebral techniques. The Goldmann applanation tonometer is mounted on a slit lamp and consists of an applanation prism that comes into contact with the patient’s fluorescein‐stained cornea using a cobalt‐blue light filter, creating lighted semicircles. Correct alignment of the semicircles is translated into a pressure reading. The Goldmann applanation method has been accepted as the criterion standard for most studies. The main limitation of the Goldmann tonometer technique is that accurate readings are not possible with cornea irregularities, scarring, or edema. The most common indentation method uses the Tono‐Pen (Figure 53.1). This is a handheld device that uses gentle manual indentations of the cornea (Figure 53.2) with the tip of the pen‐like instrument to produce electronically averaged readings of IOP. The Tono‐Pen is portable and utilizes a disposable rubber tip cover, making it ideal for the acute care setting and rapid sequential uses. The Schiotz tonometer is another common indentation tonometry method that uses a small weighted device to indent the cornea in the supine patient (Figure 53.3). The amount of indentation is measured against a calibrated weight, and the IOP is then determined. Noncontact methods that utilize puffs of air to flatten the cornea, and then measure the IOP by correlating it to the time to corneal flattening, are not typically used in the emergency department (ED). Rebound tonometers, such as the Icare Tonometer (Figure 53.4), bounce a small plastic‐tipped metal probe on the cornea and calculate the IOP based on the induction current it creates upon its return through an induction coil. The Icare Tonometer has the advantage of not requiring topical anesthetic and has even been trialed as a device that patients can use at home to monitor IOP.1 Finally, transpalpebral tonometry using the Diaton tonometer allows for IOP measurement through the upper eyelid, eliminating contact with the cornea completely. Figure 53.2 Use of the Tono‐Pen XL to measure intraocular pressure. Figure 53.3 Use of the Schiotz tonometer on a supine patient. Figure 53.4 Use of the Icare tonometer. (Used with permission of Icare‐USA.) While the Goldmann applanation method has been accepted as the criterion standard for most studies, most emergency physicians are not trained in its use. It is bulky, nonportable, expensive, and not widely available in acute care settings. Similarly, noncontact methods using puffs of air are cost prohibitive. These limitations make the search for suitable alternatives to measure IOP in the acute care setting desirable. While indentation devices (including the Schiotz and Tono‐Pen) are currently available in most EDs, newer rebound and transpalpebral tonometers are being marketed and are also within the budgetary constraints of most EDs. Are IOP measurements using the Schiotz tonometer, Tono‐Pen, Icare Tonometer, or Diaton Tonometer reliable and accurate compared to IOP measurements using the criterion standard, Goldmann applanation tonometry? Several small studies have compared IOP measurements using Goldmann tonometry against a Schiotz, the Tono‐Pen, or both. Jackson et al.2
Chapter 53
Intraocular Pressure
Background



Clinical question





Full access? Get Clinical Tree


