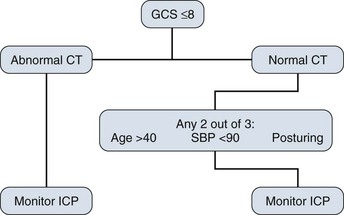
16 The history of ICP monitoring dates to 1891, when Quincke measured the cerebrospinal fluid (CSF) pressure via a lumbar puncture.1 Soon afterward, Cushing showed that as ICP increases and approaches systemic arterial pressure in an animal model, hypertension, bradycardia, and respiratory changes become evident.2 The use of continuous ICP monitoring was first described by Guillaume and Janny3 using an intraventricular catheter in 1951. Nine years later, Lundberg4 published the first systematic observations of ICP and its response to medical and physiologic interventions. Using ventricular catheters, he showed the clinical value of direct ICP monitoring and described pressure waveforms, of which the Lundberg A wave has the most practical importance in the intensive care unit (ICU). These A, or plateau, waves are characterized by a steep increase in ICP to 60 to 80 mm Hg lasting 2 to 5 minutes or longer, followed by a rapid decrease to near initial baseline pressures. This represents a pathologic response to decompensation of pressure controlling mechanisms.4–6 Since these early investigations, CSF pressure and ICP measurement have been developed and refined further. An ICP monitor is an invaluable research and clinical tool, contributing to the understanding of intracranial pathologic conditions and the assessment of therapeutic interventions. ICP monitoring can be used for patients with intracerebral hemorrhage, Reye syndrome, hepatic encephalopathy, encephalitis, stroke, hydrocephalus, near-drowning, and subarachnoid hemorrhage, but most of the clinical experience with ICP monitoring involves traumatic brain injury (TBI). In severe TBI, it is important to know if ICP is elevated. Early signs and symptoms of increased ICP include headache, lethargy, nausea, and vomiting. In critically ill patients, these clinical signs may be nonspecific and unreliable.6 In addition, the positive trend toward early intubation and sedation, if not pharmacologic paralysis, eliminates the neurologic assessment of a patient with the exception of pupils. Even papilledema, a hard physical sign of increased ICP, is rarely seen acutely in patients with TBI.7 Computed tomography (CT) is arguably the most useful diagnostic tool in patients with TBI, but may not reliably determine the ICP. ICP monitoring in severe TBI has become routine because it facilitates rational management, provides prognostic information, and improves outcomes.8–11 ICP monitoring can provide crucial information relative to cerebral perfusion pressure (CPP); detect the development or enlargement of a mass lesion, such as contusion or hematoma; facilitate the estimation of intracranial compliance; and be the only parameter to follow in a pharmacologically paralyzed patient, apart from the pupillary examination. It is rarely justifiable to treat a patient for intracranial hypertension empirically without a mechanism for measuring the effect of treatment, such as a clinical examination or ICP. There are well-defined guidelines for the use of ICP monitoring in TBI, which include patients with an abnormal CT scan and a Glasgow Coma Scale score of 8 or less after cardiopulmonary resuscitation. An abnormal CT scan is defined as one that reveals hematomas, contusion, edema, or compressed cisterns. It also is recommended to consider monitoring head-injured patients with a Glasgow Coma Scale score of 8 or less even if the head CT scan is negative if two of the following three criteria are met on admission: age older than 40, systolic blood pressure less than 90 mm Hg, or signs of posturing (Fig. 16.1).12 Although ICP monitoring can be a useful tool in the ICU, this technology has limitations. It is crucial not to assign undue weight to a normal ICP if other clinical information suggests otherwise. ICP does not always increase in the presence of midline shift.13,14 More specifically, a temporal lobe mass can herniate over the tentorial edge and cause brainstem compression without a concomitant increase in ICP.15,16 Likewise, there is not good correlation between supratentorial and infratentorial pressures,17 so it is imperative to remember that patients with a posterior fossa mass can deteriorate rapidly without a significant increase in ICP measured in the supratentorial compartment.6 ICP waveform analysis includes systolic and diastolic pressures with superimposed respiratory variation; however, the mean pressure is of practical importance. A normal adult mean ICP is 10 mm Hg or less with transient physiologic elevations above this value seen in a head-down position or during a Valsalva maneuver (see discussion of secondary injury in Chapter 67).6 The Association for the Advancement of Medical Instrumentation developed standards for ICP monitoring devices that require a pressure range from 0 to 100 mm Hg, an accuracy of ±2 mm Hg in the range of 0 to 20 mm Hg, and a maximal error of 10% between 20 mm Hg and 100 mm Hg.18 There are four basic types of clinically useful monitoring systems: ventricular catheter, subarachnoid bolt, fiberoptic device, and catheter tip strain gauge. A ventriculostomy is the gold standard for ICP monitoring. It can be inserted through a twist drill craniostomy at the bedside and can also be used to drain CSF or for the estimation of intracranial compliance. The catheter is connected to a fluid-filled system, which is connected to an external transducer. The transducer converts the measured pressure to an electrical signal, which provides a waveform and numerical value displayed on a monitor through a signal processor. A three-way stopcock is used to divert CSF from the monitor to a drainage bag if needed. This setup allows the catheter to be zeroed as frequently as necessary with the transducer positioned at the level of the center of the brain, which generally corresponds to the external auditory meatus. This system has the potential to be opened and contaminated and infected. The most significant risk of a ventriculostomy is infection; rates of 27% have been cited,10,19–22 although most reported rates are in the 1% to 10% range.21,23–26 Infection rates are similar regardless of procedure location (ICU or the operating room).20,21,27 Tunneling the catheter subcutaneously to a distant skin exit site seems to reduce the infection risk. Other risk factors for infection include irrigation of the catheter or drainage system and the presence of intraventricular blood.20,21,28 Duration of monitoring also may be a risk factor for infection. Some studies have found an increase in infection rates when ventriculostomies were left in for longer than 5 days,20,21,25 but more recent data reveal no significant reduction in infection rates when catheters were replaced before the fifth day.29 Likewise, other investigators have found no significant relationship between duration of monitoring and rate of daily infection for 2 weeks.30 The literature on the role of prophylactic antibiotics during external CSF drainage is also variable.20,26,28,31 A Brain Trauma Foundation Level III recommendation discourages routine ventricular catheter exchange as well as prophylactic antibiotics for ventricular catheter placement.32 Antibiotic-impregnated catheters have been shown to reduce infection rates33 and are being used routinely in some centers. Hemorrhage at the time of placement occurs about 1% to 2% of the time and only rarely needs to be surgically evacuated.6,25,34 A more common problem with placement is difficulty in accessing small, compressed, or shifted ventricles, resulting in malposition and a poor waveform. Although a ventriculostomy is generally considered to be the most precise and accurate method of measuring ICP,35 malfunction occurs if the ventriculostomy becomes clogged with air, blood, or debris, or if the ventricles are collapsed around the fenestrations in the catheter tip. In addition to its primary use as an ICP monitor, a ventriculostomy is commonly used in the ICU as a drain for patients with TBI or hydrocephalus. Common causes of acute hydrocephalus in an adult ICU include cerebellar stroke or hemorrhage, intraventricular hemorrhage, and aneurysmal subarachnoid hemorrhage. A common and often debated concern regarding CSF drainage with a ventriculostomy is that it can cause subfalcine herniation in the presence of a hemispheric mass or upward herniation of the cerebellum in the presence of an infratentorial lesion.36 Under these circumstances, we believe that surgical decompression of the primary mass also should be considered. Another potential risk of ventricular catheter insertion is aneurysmal rebleeding37 after an acute subarachnoid hemorrhage. Our group’s opinion is that the benefit of treating hydrocephalus with high ICP far outweighs the small, potential risk of aneurysmal rebleeding, and we have a low threshold for placing a ventriculostomy in these patients. The subarachnoid bolt technique for ICP monitoring was developed because of concern about the infection rate associated with ventriculostomies, and because small ventricular size after head trauma often makes catheter insertion difficult.38 A subarachnoid bolt is a self-tapping metal or plastic tube that is screwed into a twist drill craniostomy at the bedside. The dura at the base of the bolt is perforated with a spinal needle to allow CSF to fill the bolt, which is connected to pressure tubing filled with preservative-free (nonbacteriostatic) saline that leads to an external transducer leveled to the ear. In contrast to a ventriculostomy, the subarachnoid bolt is only a monitoring instrument; CSF is not withdrawn from it. It usually provides a reliable ICP waveform and pressure reading, but is susceptible to error if the dural perforations become obstructed with blood or debris, or if brain swelling obliterates communication with CSF. Uncapping the bolt to flush debris with 0.2 mL of preservative-free saline solution can restore accurate ICP readings and is unlikely to cause dangerous ICP elevation.39 The subarachnoid bolt tends to underestimate ICP, particularly when ICP is elevated.39,40 Because the subarachnoid bolt measures the local ICP at the surface of the hemisphere, it can be inaccurate if a pressure gradient is present between the left and right supratentorial compartments.19 The existence of compartmental pressure differences has been debated, but such gradients can occur between the left and right hemispheres or the supratentorial and infratentorial compartments and sometimes are only transient.19,41–43 This is an important phenomenon to consider, and if a discrepancy exists between an apparently normal ICP and the patient’s clinical condition or CT scan or both, treatment of elevated ICP may be warranted. The infection risk for subarachnoid bolts is extremely low, and infections are nearly always superficial and rarely involve the brain or meninges.20 No local or systemic infection was reported with the use of subarachnoid bolts in 124 comatose children.44 Risk of subarachnoid bolt infection is increased when the bolt is opened and flushed to improve the waveform.20 Subarachnoid bolts are rarely associated with brain injury; however, intracerebral hematoma may occur45 if there is a mishap with the drill, or if the needle used to puncture the dura is passed too deeply. Since the introduction of fiberoptic catheters, subarachnoid bolts are being used less often. Fiberoptic ICP monitors use miniature transducers that are coupled via fiberoptic cables to an external instrument. These monitors can be placed at the bedside through a standard twist drill craniostomy or through a smaller opening made with a 2.71-mm bit. The transducer is incorporated into the end of a tube and can be used alone or in combination with a ventriculostomy. Fiberoptic systems operate by projecting light through an optic fiber to a miniature, displaceable mirror in the catheter tip.46 The amount of light reflected to a collecting optic fiber depends on the mechanical displacement of the mirror, which is a function of ICP. Fiberoptic devices can be inserted into the lateral ventricle, the brain parenchyma, or the subdural space. The greatest advantage of fiberoptic catheters is that they do not require fluid coupling for pressure transduction, which avoids the problems of waveform dampening and artifacts from poor coupling. Because they do not require fluid coupling, there also is less opportunity for contamination. The mechanism that does the actual pressure transduction is what is inserted into the patient; the system functions independent of head position, and the monitor is zeroed once before it is placed. This feature also is a disadvantage because the transducer cannot be recalibrated to zero after insertion. System accuracy compared with a ventriculostomy has been shown in the subdural space, brain parenchyma, and ventricles, although the parenchymal fiberoptic pressures may consistently exceed ventriculostomy pressures by nearly 10 mm Hg.47–49 The fiberoptic device has an average daily drift of ±0.6 mm Hg. Over a 5-day period, there is an average drift of 2.1 mm Hg with a maximal drift of ±6 mm Hg. This drift over time may be enough to necessitate replacement if ICP monitoring is required for more than 5 days.6,49,50 Complications with the use of fiberoptic catheters relating to hemorrhage51,52 and infection51 have been reported, but our experience is that clinically relevant problems are unusual, particularly with intraparenchymal monitors. We do exercise caution, however, in patients with coagulopathy. The catheter tip strain gauge consists of a miniaturized solid-state pressure sensor mounted in a titanium case at the tip of a long, thin, flexible nylon tube. The transducer tip contains a silicon microchip with diffuse piezoresistive strain gauges that connect to tiny wires that travel the length of the tube. This is a small wire with a diameter of 1.2 mm that can be placed at the bedside. It can be incorporated into a ventricular catheter and used in any intracranial space. This device is accurate with a low daily drift range between −0.125 mm Hg and +0.110 mm Hg. It shares many of the advantages and disadvantages of fiberoptic devices,6,53,54 but we have found it more cumbersome to place and secure through a bedside twist drill craniostomy.
Intracranial Monitoring
Intracranial Pressure Monitoring
Ventricular Catheter
Subarachnoid Bolt
Fiberoptic Intracranial Pressure Monitors
Catheter Tip Strain Gauge
Anesthesia Key
Fastest Anesthesia & Intensive Care & Emergency Medicine Insight Engine