Fig. 80.1
CT scan images of small bowel obstruction. (a) Representative axial section of CT scan of the abdomen and pelvis with PO and IV contrast showing dilated, fluid filled small bowel. (b) Representative coronal section of CT scan for the same patient showing dilated, fluid filled small bowel consistent with small bowel obstruction
Question
How do you manage a patient with a small bowel obstruction?
Answer
Since this patient had no signs of intestinal ischemia (fever, leukocytosis, tachycardia unresponsive to fluids, peritonitis), intestinal perforation (no pneumoperitoneum), a closed loop obstruction or hernia defect and had a history of prior abdominal surgery suggesting an etiology of adhesive small bowel disease, he was initially managed non-operatively with IVF resuscitation, NPO and nasogastric (NG) tube decompression. The NG tube initially evacuated 1.5 L of gastric and bilious fluid.
Over the course of the next 3 days, the NG tube output remained elevated but was more gastric in nature. He remained with only minimal abdominal tenderness but he was not passing gas per rectum or having bowel movements. As a result, laparotomy with lysis of adhesions was recommended for treatment of persistent small bowel obstruction and performed on hospital day 4. During the laparotomy, a combination of extensive moderate and dense adhesions was identified that twisted the bowel in a partially obstructed, but not ischemic, fashion. After lysis of adhesions, the small bowel was decompressed and its contents evacuated into the NG tube. The NG tube was removed on post-op day (POD) #1, diet started on POD#2, gas passed and bowel movement occurred on POD#3, and he was discharged to home on POD#5 once INR was therapeutic.
Standard Approach to Management
Small bowel obstruction (SBO) is most commonly due to adhesive disease, Crohn’s disease, tumors or hernias [1]. The primary concern with SBO is bowel ischemia or necrosis. Since there are no physical exam findings, lab values or imaging tests that will confirm the presence of ischemia, it is a combination of these signs, symptoms and tests that must be evaluated to determine if laparotomy is necessary. As stated in the scenario above, leukocytosis, tachycardia unresponsive to fluid administration, acidosis and peritonitis are all concerning for intestinal ischemia [2, 3]. The presence of pneumoperitoneum on imaging signifies bowel necrosis and perforation and should prompt emergent exploration. A closed loop obstruction on CT imaging with focal peritonitis should prompt exploration as well. With the increased frequency of CT use, concerning imaging findings include portal venous gas, mesenteric edema and inflammatory stranding that may favor earlier rather than later exploration.
Patients with SBO more commonly present without an absolute indication for exploration (Fig. 80.2). In patients without immediate concern for bowel ischemia, bowel rest with NPO and NG tube decompression, fluid resuscitation, correction of electrolyte abnormalities and minimization of narcotics are trialed for a few days. Approximately 75 % of SBOs treated non-operatively will not require surgery during that admission [4]. Any evidence of worsened pain, tachycardia, acidosis or leukocytosis necessitates laparotomy. Otherwise, patients can be successfully managed non-operatively for 3–4 days until signs and symptoms of SBO resolve with restoration of intestinal function. Predictive models for the need for laparotomy using presenting symptoms, physical exam, lab values and CT imaging findings have been described but are not yet fully validated [5, 6].
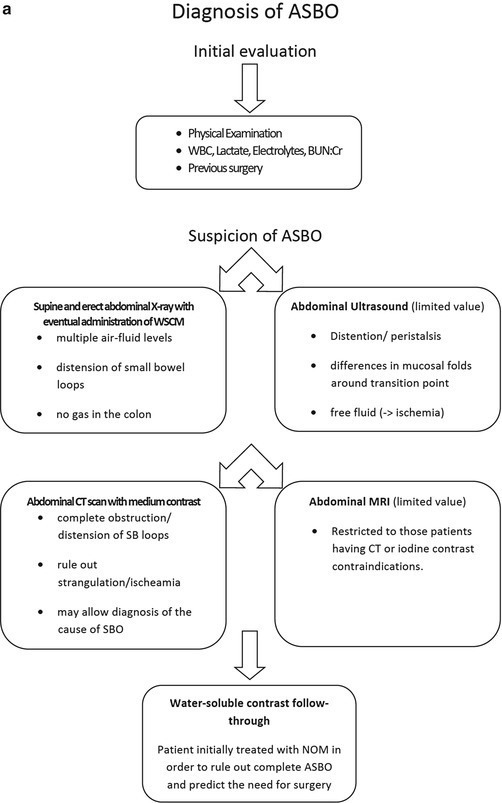
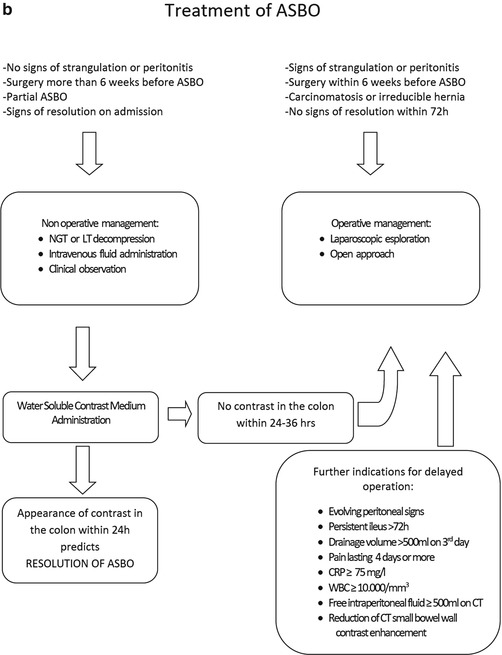
Fig. 80.2
Evidence-based Algorithm for Diagnosis (a) and Treatment (b) of Adhesive SBO (ASBO) (From DiSaverio et al. [7]. © Di Saverio et al.; licensee BioMed Central Ltd. 2013 [Creative Commons Attribution License])
Evidence Contour
Timing of Operating for SBO
An old surgical dogma was to never let the sun set or sun rise on a SBO. This is no longer the case. However, when to operate for a SBO continues to challenge surgeons. For patients with prior abdominal surgery who most likely have an adhesive SBO, a trial of 48–72 h of non-operative management is successful in relieving the obstruction in ~75 % of cases [7].
Recently, the use of water-soluble contrast via NG tube or by mouth has been used to both treat and assess patients with adhesive small bowel disease [8, 9]. Essentially, patients are given a small volume of water-soluble contrast and serial abdominal plain films are obtained. Passage of contrast into the colon within 24 h of administration indicates resolution of the SBO and trials of a diet can ensue. This technique leads to shorter lengths of stay [10].
Management Differences Between Small and Large Bowel Obstruction
The case in this chapter illustrates the course of care for SBO. SBO is much more common than large bowel obstruction (LBO). Although the presenting symptoms may be similar, the diagnostic work up and treatment are different. Adhesive disease does not normally lead to large bowel obstruction with the greatest concern with large bowel obstruction being cancer.
LBO is an emergency condition that requires early identification and intervention. Complete LBO, closed loop obstruction, evidence of colonic ischemia and volvulus commonly require emergency surgical intervention.
Other unique causes of large bowel obstruction include cecal or sigmoid volvulus, colonic ileus (Ogilvie’s syndrome), toxic megacolon with Clostridium difficile infection, diverticular stricture and fecal impaction [11]. The clinical scenario for each of these potential causes of large bowel obstruction should help in delineating the cause and initial management steps. Also unique to patients with large bowel obstruction, especially in those who are debilitated and cannot undergo surgery [12] or who need to have an acute obstruction temporized [13], is the use of colonic stents to bypass an area of stricture or obstruction [14].
Management of Acute Small Bowel Obstruction in a Patient with No Prior Abdominal Surgery or Pathology
Less than 10 % of cases of small bowel obstruction will be present in patients without prior abdominal surgery. With the known etiologies of small bowel obstruction being adhesions, inflammatory bowel disease and hernias, an SBO in a virgin abdomen presents a clinical conundrum. Unfortunately, there is little evidence available to guide clinical management. Currently, unless the patient clearly has evidence of an infectious or inflammatory etiology for the obstruction, exploration with either laparoscopy or laparotomy is recommended given the concern for an underlying malignancy. However, recent data would suggest that up to 75 % of laparotomies for SBO in a virgin abdomen are due to adhesions [15]. Regardless, until more data is available, we recommend either laparoscopy or laparotomy for the evaluation of SBO in patients with a virgin abdomen and no obvious infectious or inflammatory source.
Related posts:






Full access? Get Clinical Tree


