CHAPTER 18

INJURY PREVENTION
Webster defines the term accident as “an unforeseen and unplanned event or circumstance” and specifically when related to an injury as “an unexpected happening causing loss or injury which is not due to any fault or misconduct on the part of the person injured.”1 While this term is commonly used when talking about unintentional injury in both the medical community and lay press, it is a misnomer. “Accidents” are actually injuries that occur under predictable and preventable circumstances. Injuries result from physical damage sustained following exposure to harmful agents, such as heat, electricity, mechanical energy, radiation, and poisons. In the United States, 59 million or 1 in 4 Americans suffer an injury annually. This results in 36 million emergency department visits and nearly 2.9 million admissions each year.2 Injuries are also a significant cause of mortality. Unintentional injury is the fourth leading cause of death overall, accounting for over 140,000 deaths (6.5% of all deaths) annually. In children, adolescents, and adults in the 1–44 age group, it is the leading cause of death.3 When considering other leading causes of death such as cancer, heart disease, congenital abnormalities and HIV, unintentional injury accounts for more death and years of potential life lost before the age of 75 than the other leading causes of death combined.3
Death following trauma occurs in a predictable, trimodal distribution (Fig. 18.1). As depicted in the graph, more than half of the deaths occur within the first hour following injury. Particularly in individuals sustaining a head injury, those that do survive to definitive care often die from their injuries despite adequate care. As a result, it is clear that trauma prevention efforts are the only mode of injury prevention that can impact this population of victims.
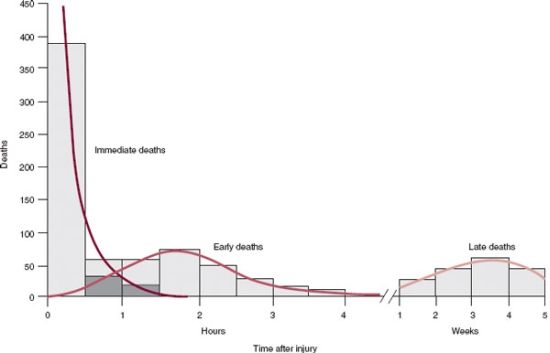
FIGURE 18.1. The trimodal distribution of trauma deaths as described in Trunkey DD. Trauma. Sci Am. 1983;249;28. (Reprinted from Feliciano D, Mattox K, Moore E. Trauma. 6th ed. New York: McGraw-Hill; 2008, with permission).
The following chapter describes the early development of injury prevention, key thinkers in early prevention efforts, and the contribution the field of epidemiology has made to injury prevention. Attention is then focused on key principles that should be considered when developing injury prevention programs with special consideration given to the assessment of injury prevention effectiveness. Finally, the chapter provides specific examples where these principles have been successfully applied to both unintentional and intentional injury prevention.
FOUNDATIONS OF INJURY PREVENTION
An appropriate starting point for any discussion on injury prevention is John Gordon. In the 1940s, John Gordon first described injuries from an epidemiological perspective. He noted that, like other disease processes, unintentional injury occurs in predictable patterns. Specifically, he hypothesized that injuries were a result of an interaction between the host, the agent, and the environment.4 This “epidemiological triad” forms the basis of modern epidemiological studies. While it is true that injuries affect specific individuals, studying patterns of injury across different social groups is crucial to prevent injury at a population level.
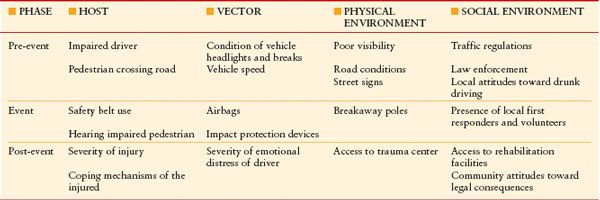
Whereas John Gordon laid the foundations for the beginning of injury prevention research, the first true leader in the field was William Haddon Jr. Realizing that injuries result from a transfer of energy from the vehicle to the host (human body), he expanded Gordon’s epidemiological triad and formulated Haddon’s Matrix. Haddon’s matrix is best described as a grid with three rows and four columns. Each row represents different phases of an injury: pre-event, event, and post-event. The four columns represent different factors that influence the severity of the injury: host, vector, physical environment, and social environment. In the pre-event phase, each of the four factors influences the likelihood that an event will occur. In the event phase, the factors interact to influence the severity of the event. Lastly, in the post-event phase, each factor determines the overall outcome.5 Consider an example where an intoxicated driver strikes an elderly pedestrian at night in a rural community (Table 18.1).
TABLE 18.1
HADDON’S 10 STRATEGIES TO PREVENT AND CONTROL INJURY
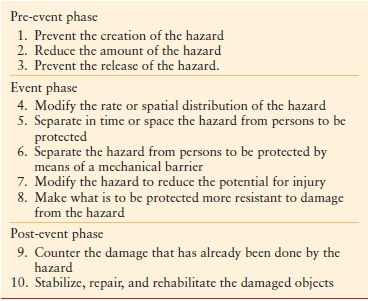
As a conceptual model, Haddon’s Matrix has been an invaluable tool used in injury prevention. In addition, Haddon later went on to develop 10 different approaches specifically targeted to prevent or control human injury. Like the matrix, they can be broken down into three phases: pre-event, event, and post-event. In brief, the 10 general strategies with examples are5: (Table 18.2).
- Prevent the creation of the hazard. Example: Laws to prevent the manufacture of certain poisons, drugs, weapons.
- Reduce the amount of the hazard. Example: Speed limits, boating regulations, firework laws.
- Prevent the release of the hazard. Example: Trigger locks for guns, nuclear waste management programs.
- Modify the rate or spatial distribution of the hazard: Example: Antilock brakes, airbags, seat belts.
- Separate, in time or space, the hazard from persons to be protected. Example: Isolation units in hospitals, pedestrian walkways.
- Separate the hazard from persons to be protected by means of a mechanical barrier. Example: Exam gloves, helmets, hazardous material containers.
- Modify the hazard to reduce the potential for injury. Example: Medications with fewer side effects, guardrails, guards on hand saws.
- Make what is to be protected more resistant to damage from the hazard. Example: Immunizations, fire resistant clothing for children, earthquake resistant buildings.
- Counter the damage that has already been done by the hazard. Example: Trauma systems, disaster response teams.
- Stabilize, repair, and rehabilitate the damaged objects. Example: Critical care medicine, reconstructive surgery, physical therapy.
TABLE 18.2
EXAMPLE OF INTERACTIONS IN HADDON’S MATRIX
In the 1960s, Haddon noted that “It has been the consistent experience of public health agencies concerned with the reduction of other causes of morbidity and mortality that measures, which do not require the continued, active cooperation of the public, are much more efficacious than those that do.”5 The term “active intervention” now serves to describe injury prevention efforts that require people to perform an act or change in behavior such as putting on a seat belt or wearing a bicycle helmet. A “passive intervention” then is one in which no action on the part of those being protected is required. Airbags are an example of a passive intervention. Intuitively, it makes sense that passive interventions are more efficacious in terms of preventing morbidity and mortality as the prevention is automatically built into the design of the intervention.
However, it is important to note that passive interventions usually require action on the part of society as a whole. As an example, in the late 1960s, to protect the public from unreasonable risk of injury following motor vehicle crashes (MVCs), the Federal Motor Vehicle Safety Standards (FMVSS) were put in place. The FMVSS are a set of regulations that describe the minimum safety performance requirement for motor vehicles, which must be met by all car manufactures.6 Under the supervision of the National Highway Traffic Safety Administration, it has been estimated that approximately 10,000 to 30,000 lives per year have been saved since its implementation.7,8
CLASSIFICATION OF INJURY PREVENTION
It is clear that William Haddon has made notable contributions to the field of injury prevention. Through the interactions between phases and factors, Haddon’s matrix is the foundation for newer concepts: primary, secondary, and tertiary prevention.9 Primary prevention is described as the complete elimination of the hazardous event. Consider scald burns in children as an example. Young age is associated with an increased risk of scald injury.10,11 Several studies have demonstrated that there is a clear relationship between water temperature and scald injury severity. Full-thickness burns can occur between 2 and 5 seconds at 60°C, and between 10 and 30 seconds at 55°C. At 52°C, 3 minutes of exposure is required to produce burns.12,13 Logically, most scald burns due to tap water can be prevented by keeping the temperature in hot water heaters to 52°C or less. In 1983, Washington State passed a legislation requiring new water heaters to be set at 49°C. It also called for warning labels on water heaters, and annual notices for customers, homeowners, and landlords describing energy savings associated with lower water temperatures.14 This legislation was extremely effective, as admissions for tap water scalds declined by 56% in two teaching hospitals in Washington state. More states adopted this legislation and since then scald-related death has decreased by half for all age groups and by 75% for children.15
While primary prevention efforts serve to eliminate the potential for injury before it occurs, this is not always possible. Secondary prevention minimizes the amount of injury that occurs when the event cannot be prevented. In a MVC, the most significant causes of injury occur during ejection, or collisions within the interior of the vehicle. Devices to dissipate kinetic energy in a more controlled fashion are designed to prevent this type of injury. There is little doubt that one such device, the seat belt, has saved thousands of lives (see following section on seat belts). A somewhat more controversial secondary prevention device is the airbag. Initially developed in the 1950s, first-generation airbags were made of nylon and were designed to deploy following a specific change in velocity. In 1989, the National Highway Traffic Safety Association (NHTSA) mandated the use of either driver airbags or automatic seat belts and by 1998 the NHTSA expanded this to include the installation of both driver and passenger airbags in all new cars. As a result, new patterns of injury associated with airbag deployment emerged. Particularly in children, there was an increase in facial fractures, cervical spine injuries, odontoid fractures, and extremity fractures in crashes with airbag deployment.16–18 There was also an increase in both mild and moderate head injury when airbags are deployed.19 As a result, second-generation airbags or “depowered” airbags are now mandated in new vehicles. Williams et al. has since reevaluated injuries associated with second-generation airbags and found that, when compared to no restraint device, airbags were associated with decreased odds of having a brain injury, or abdominal injury and had a decrease in infectious morbidity, hospital resource use, and mortality.20
Restraint devices have saved thousands of lives and are an excellent example of secondary prevention. Tertiary prevention can be thought of as efforts that will optimize the outcome after an injury has occurred. An example is the development of trauma centers and the trauma triage system. In the early 1970s, trauma patients were transported to the nearest hospital regardless of institutional resources. As the concept of specialized trauma centers evolved, in 1976 the American College of Surgeons (ACS) developed a document entitled “Resources for Optimal Care of the Injured Patient.”20 This resource outlined mechanistic, physiologic, and anatomic criteria that warranted transport to a trauma center following an injury. After its implementation, the first reports of improved morbidity and mortality associated with the use of specialized trauma centers emerged.22 The American College of Surgeons Field Triage System is an extension of the “Resources” guidelines. This scheme has four steps23:
- Assessment of vital signs, and level of consciousness.
- Assessment of anatomic injury.
- Assessment of the mechanism of injury with specific search for evidence of high-risk collisions (e.g., auto vs. pedestrian, motorcycle crash >20 mph).
- Assessment of special patient or system considerations (e.g., age, burns, pregnancy).
The beneficial result of improved trauma systems is also considerable.24 As an example, when controlling for other factors, in a study comparing mortality in Level I trauma centers versus non-trauma centers across 14 different states, MacKenzie et al.25 found that the risk of death was considerably lower when patients were cared for at a trauma center.
TYPES OF PREVENTION EFFORTS
Whether primary, secondary, or tertiary prevention is the intent, the implementation of injury prevention strategies can be thought of according to the four “E’s:” (1) Education, (2) Enforcement and legislation, (3) Engineering, (4) Economics. Education and efforts to promote behavioral change in high-risk groups have classically been the cornerstones of injury prevention design. This is based on the principle that knowledge will lead to behavioral changes. An example of a successful educational program is the “Just say no” campaign. As a part of the advertising strategy for the US “War on Drugs” in the late 1980s and 1990s, the slogan “Just Say No” was championed by the then first lady Nancy Reagan. When approached by an elementary school student who asked what the first lady would do if she was offered an illegal drug, Mrs. Reagan replied “Just say no.” The phrase caught on immediately and led to the formation of thousands of “Just say no” groups across the United States. Mrs. Reagan visited drug rehabilitation and prevention institutions, and enlisted the help of several community groups, including the Girl Scouts of America and the Kiwanis Club to get the message out that drugs are harmful. “Just say no” also became a part of pop culture, appearing on popular television programs, in music videos, and on billboards across the United States.26 While it is difficult to infer a causal relationship, the National Institute on Drug Abuse reported a significant decrease in marijuana, cocaine, and heroin use amongst high school students in the 1980s.27
Enforcement and legislation are also important in injury prevention. Despite adequate educational attempts, there are always individuals who will resist change, even when they may benefit from the improved outcome. As an example, despite considerable evidence to support the fact that restraint belts save lives and prevent serious injury, seat belt usage in the United States is not 100%. Currently, 30 states and the District of Columbia have primary enforcement laws where police may stop vehicles solely for occupants not wearing seat belts.28 However, in states where primary enforcement laws are in place, 86% of occupants wear seat belts versus 78% of occupants in states where seat belt use is not enforced.29
Engineering and technology encompass a wide variety of topics, and may have the largest impact on injury when considering long-term benefits. Examples where engineering has been useful include the development of trigger locks on firearms, earthquake resistant buildings, and built-in protective devices on manufacturing equipment. Following the 1994 earthquake that struck Northridge California, a population-based cohort study was conducted to determine factors associated with increased physical injury. This study was unique in that it sought to examine how seismic risk factors, patient demographics, and building characteristics simultaneously interacted to produce injury compared to an exposure matched cohort. When controlling for other factors, building and seismic factors were identified, which independently increased risk of injury.30 This information was useful to give back to engineers to target points of intervention.
Funding for injury prevention programs is generally inadequate. Within the community, there is a finite supply of volunteer services, not-for-profit organizations, and donations. Economic incentives (or penalties) can serve to reinforce legislative efforts when patient participation is required for successful prevention. Insurance companies, for example, have data on risk-taking behavioral patterns. Discounted premiums can then be offered to groups with lower risks (i.e., High school drivers who meet a minimum GPA). In a different example, consider the use of child car seats. It is well recognized that, particularly in the 0–4 age group, infants and young children do not fit into adult-sized seat belts and can suffer devastating injury if unrestrained in a MVC. All 50 states currently require child car seats. The success of this legislation is seen in the reduction in childhood deaths related to motor vehicles. When compared to 1994, where primary enforcement of child car seats was not mandatory, there were 682 deaths in the United States from MVCs compared with 471 deaths in 2006.3,31
EVALUATION OF INJURY PREVENTION STRATEGIES
Whether the prevention strategy is education, legislation and enforcement, engineering or economic, critical evaluation of the effectiveness of a program is essential. Outcome assessment is vital to continue to fund strategies with proven benefit and is likewise useful to identify those that do not work. Many educational efforts consume a considerable amount of community resources and have excellent face validity, yet there may be little or no effect on outcomes. Alternatively, the outcomes affected may be only short-term or secondary endpoints. Educational programs teaching young children pedestrian safety illustrate this point. In a large meta-analysis that included 15 randomized controlled trials, which looked at the effectiveness of pedestrian safety education programs in preventing pedestrian versus motor vehicle collisions, education resulted in improved children’s knowledge of road dangers and some changes in road crossing behaviors. However, the authors also concluded that the targeted “safe” behaviors in these trials were not necessarily related to decreased pedestrian injury risk.32
In an ideal situation, the outcomes an investigator wishes to prevent are those injuries that lead to death or major disability. In many situations, this is not possible. Injury outcomes can be described in a hierarchy. At the top are the serious outcomes that are desirable to prevent, yet difficult to access for change. Traveling downward are those that are more easy to assess for change, but of lesser importance in the prevention of serious outcomes.33 (Fig. 18.2):
- Death
- Inpatient admissions following trauma
- Injuries treated in the outpatient setting
- All injuries
- Behavioral change
- Self-reported behavior
- Measures of knowledge, attitudes, or intensions

FIGURE 18.2. Hierarchy of outcomes associated with injury prevention techniques as described by Maier R, Mock C. Chapter 3. Injury prevention (Chapter). In: Feliciano D, Mattox K, Moore E, eds. Trauma. 6th ed.
The type of outcome measure selected for assessment depends on the population characteristics, type of intervention planned, and resources (particularly monetary) provided to the team. Clearly, all interventions should seek to impact those outcomes with the biggest impact (i.e., trauma resource utilization or mortality). This is not always possible for smaller projects. In those cases, the appropriate selection of a surrogate outcome measure with proven validity in similar situations may be beneficial. Regardless of the measure chosen, outcome assessment is crucial when developing an intervention.
THE PREVENTION OF UNINTENTIONAL INJURIES
MVC-related injures remain the leading cause of death for people between the ages of 1 and 34. In 2006, the total number of people killed in an MVC was 43,664, with vehicle-related deaths contributing 35.9% of the total unintentional mortality overall.3 However, there have been many recent advances in automotive safety that have contributed to declining mortality over the last several years. The following section outlines some for individual discussion.
SAFETY BELTS, AIRBAGS, AND CHILD CAR SEAT RESTRAINTS
Saving an estimated 15,000 lives per year, seat belts are extremely effective in preventing injuries sustained in MVCs.34 In 2001, as a part of the CDC’s Motor Vehicle Injury Prevention program, the Task Force on Community Preventive Service concluded that seat belt laws and primary enforcement were effective and strongly recommended. The task force went on to recommend a goal of 92% overall seat belt use by 2010. In 2006, the overall prevalence in the United States was 82.4% with only four states achieving seat belt use rates >90% in self-reported surveys.35 Interestingly, the 15 states with the highest levels of seat belt use also had primary enforcement laws. This is in contrast to 14 of the 15 states with the lowest levels of seat belt use that only had secondary enforcement or no enforcement at all.35







Full access? Get Clinical Tree


