Chapter 173 The prevalence of acute gastroenteritis in children has not changed much during the past four decades, but the mortality has declined sharply.1 Although dehydration is the most common complication of acute infectious diarrhea, one of the most important reasons for the decline in mortality has been the increasing international support for the use of oral rehydration solutions (ORSs) as the treatment of choice for acute diarrhea. However, in emergency departments (EDs) across the nation, intravenous therapy is still routinely used for treatment of volume depletion due to infectious diarrhea. A few reasons that EDs still routinely use intravenous therapy instead of oral rehydration are the misconceptions that intravenous therapy is more effective, that it takes less time, and that it poses little risk. However, some potential serious complications have emerged as a result of overuse of parenteral rehydration. These include local complications from intravenous infiltrations (hematoma, thrombosis, phlebitis, postinfusion phlebitis, thrombophlebitis, infiltration, local infection, extravasation, and vasospasm) and systemic complications from overly aggressive replacement of volume deficits leading to central nervous system sequelae and pulmonary edema. In many situations, diarrhea-related volume depletion can be treated by enteral replacement by oral intake or delivered by nasogastric or orogastric tubes. In 2008, of the estimated 8.795 million deaths in children younger than 5 years worldwide, infectious diseases caused 5.970 million (68%) of these deaths. The largest percentages were due to pneumonia, diarrhea, and malaria (in decreasing order). Diarrhea was responsible for 15% or 1.336 million of these deaths.2 Regional differences in resources, epidemiology, underlying general health status of the population, and availability of safe food and water affect the actual disease burden. In the United States, acute gastroenteritis historically accounts for approximately 10% of hospital admissions of children younger than 5 years, estimated at 220,000 admissions per year; 300 to 400 deaths per year are caused by diarrhea, most occurring in the first year of life.2,3 In the United States, acute gastroenteritis is responsible for 3.7 million physician visits, 135,000 to 220,000 pediatric admissions (approximately 10% of total hospitalization for children younger than 5 years), and 150 to 300 deaths among children younger than 5 years.3–5 Costs to society are significant, with approximately one billion dollars in total costs attributed to rotavirus alone.6,7 The incidence of diarrhea in children younger than 3 years has been estimated to be 1.3 to 2.3 episodes per child per year; rates in children attending daycare centers are higher. Pediatric death due to diarrhea is related to severe dehydration and associated complications. Improvements in recognition and treatment of dehydration have prevented many deaths in the United States. Risks factors for death from diarrhea include age younger than 1 year; birth weight less than 2500 g; African American, Hispanic American, or American Indian ethnicity; immunocompromise; and illness during winter months.3,4 In the United States, viruses are responsible for most cases of acute infectious diarrhea. Rotavirus, norovirus, astrovirus, and enteric adenovirus have been recognized as the most common agents responsible for viral diarrhea in children. Bacteria cause approximately 7 to 10% of cases of acute infectious diarrhea. The most common bacteria are Escherichia coli, Campylobacter species, Salmonella species, Shigella species, and Yersinia enterocolitica. Clostridium difficile is also seen as a cause of infectious diarrhea, especially in patients who have recently taken antibiotics and hospitalized patients. Parasitic causes of infectious diarrhea are uncommon in the immunocompetent patient, but they can occur. The most common parasitic organisms are Cryptosporidium, Giardia, and Entamoeba histolytica.8–11 Infectious diarrhea in children is most often contracted through the fecal-oral route and through poor food-handling practices. Daycare centers remain a main source of cases, with infection spread by diaper handling, fecal-oral transmission, and sharing of toys. Causative agents may be endemic, epidemic with food- and water-borne outbreaks, or sporadic. For most agents, a large inoculum is required to transmit the illness. The exceptions are Campylobacter, Giardia, and Shigella, for which 10 to 200 organisms are sufficient to cause disease. Some groups are at higher risk for acquiring infectious diarrhea and suffer greater clinical consequences. Among these are premature infants, young infants (<3 months), and patients who are immunosuppressed or malnourished or who have a chronic disease. Recent hospitalization, treatment with broad-spectrum antibiotics, and travel to developing countries are additional risk factors. Definitions.: Secretory diarrhea is the result of increased intestinal secretion caused by a variety of mechanisms. In the case of Vibrio cholerae, an enterotoxin causes an increase in cyclic adenosine monophosphate (cAMP) in the endothelial cell, resulting in increased chloride and bicarbonate secretion. Clinically, secretory diarrhea is often characterized by the absence of expected reduction in stool volume with fasting, a stool pH above 6, and the absence of reducing substances in the stool. Other bacteria that produce enterotoxins include Salmonella, Shigella, E. coli, and C. difficile. Before the diagnosis of acute infectious diarrhea is established, other potentially life-threatening illnesses that can be manifested with diarrhea with or without vomiting should be excluded. This can usually be accomplished with a thorough history and physical examination (Tables 173-1 and 173-2). Table 173-1 Common Causes of Vomiting in Children Table 173-2 Common Causes of Diarrhea in Children A variety of viruses, bacteria, and protozoa can cause acute infectious diarrhea in children (Table 173-3). In developed countries such as the United States, viral causes predominate. In countries in which access to clean water and food supply is limited, bacterial agents contribute the major portion of the morbidity and mortality associated with infectious diarrhea. Table 173-3 Common Causes of Infectious Diarrhea Rotavirus is the leading cause of diarrhea worldwide among children younger than 5 years.12 In the United States, rotavirus is responsible for 410,000 office visits, 205,000 to 272,000 ED visits, and 55,000 to 77,000 hospitalizations each year. This virus is endemic and accounts for nearly one third of the cases in children with diarrhea. The number of cases of rotavirus infection peaks in the winter and spring. Rotavirus causes acute illness with vomiting and diarrhea that may or may not be associated with fever. The diarrhea is watery, and the volume may be large enough to result in significant and rapid intravascular volume depletion. Rotavirus also may cause symptoms of an upper respiratory tract infection. Most infections are transmitted person to person through the fecal-oral route. There is also evidence that it may be transmitted through respiratory secretions as airborne droplets. The incubation period is 1 to 3 days. Postinfection excretion may be prolonged up to 21 days after the onset of symptoms in the immunocompetent patient.13 Rotavirus selectively destroys the villus tip cells in the small intestine, leading to malabsorption and diarrhea. A proliferative response occurs, producing an abundance of incompletely differentiated cells in the gut mucosa. In the healthy host, repair of the epithelium and differentiation of the immature brush border take approximately 3 to 5 days and occur without specific intervention. In the chronically ill or malnourished child, the infection may lead to complications beyond the usual brush border injury. Failure to repair the epithelium leads to the vicious circle of malnutrition and progressive epithelial injury.13 Diagnosis is made by demonstration of antigens in stool specimens by enzyme immunoassay. Modern assays have up to 97% sensitivity and 97% specificity for rotavirus antigens in human stool. The test can be performed on undiluted stool without special preparation. Results are usually available within 24 hours.13 An effective vaccine was available for a short time (1998-1999) until it was noted to be associated with increased risk of intussusception, usually occurring 3 to 20 days after administration. This vaccine was subsequently withdrawn from the U.S. market.14 Until recently, only two orally administered live virus vaccines were licensed for use among infants in the United States. RotaTeq vaccine was licensed in 2006 as a three-dose series, and in 2008 Rotarix, a live oral human attenuated vaccine, was licensed as a two-dose series for infants. The American Academy of Pediatrics does not express a preference for either vaccine. To date, no association with intussusception has been reported.15,16 Preliminary surveillance data from the Centers for Disease Control and Prevention (CDC) have noted a 64% decrease among rotavirus-positive test results in the first year after vaccine release.17 Recently, a new vaccine was introduced, the RV1 vaccine; studies in Brazil and Mexico show the risk of intussusception after RV1 vaccine to be 1 in 51,000 to 68,000. The authors concluded that this increased risk results in an annual excess of 96 hospitalizations and that this risk is outweighed by the benefit of the vaccine, which prevented 80,000 admissions and 1300 deaths.17 Noroviruses (previously known as Norwalk-like viruses) are the second most common cause of childhood acute infectious diarrhea. Norovirus accounts for approximately 12% of severe gastroenteritis among children younger than 5 years. In the United States, norovirus is responsible for more than 235,000 clinic visits, 91,000 ED visits, and 23,000 hospitalizations for children younger than 5 years.18,19 Infection can occur year-round and in any age group but is most common during the colder months of the year. This virus causes the abrupt onset of watery diarrhea with or without vomiting. It is often accompanied by abdominal cramps and nausea. It is a self-limited disease, lasting 2 or 3 days. This virus can be transmitted person to person by the fecal-oral route as well as through contaminated food and water sources. In the United States, norovirus accounts for more than 90% of community outbreaks associated with viral gastroenteritis, which occur in all age groups. Common-source outbreaks in long-term care facilities contribute significantly to morbidity and mortality among the residents. In addition, these agents most commonly are associated with outbreaks of acute gastroenteritis on cruise ships and in schools and hospitals. The incubation period is 12 to 48 hours, and the excretion of the virus lasts 5 to 7 days after the onset of symptoms in approximately 50% of infected people. In about 25% the excretion of the virus can be up to 3 weeks, and asymptomatic excretion can be longer in the immunocompromised.20 Astrovirus infections occur mostly in children younger than 4 years; cases peak in the late winter and early spring in the United States. The illness is characterized by diarrhea of short duration (a few days) accompanied by vomiting, fever, and occasionally abdominal pain. The incubation period is 1 to 4 days and transmission is person to person by the fecal-oral route. Viral shedding may begin a day before symptoms start and can continue for several days after cessation of diarrhea. However, asymptomatic shedding has been seen to last up to several weeks after the symptoms of the illness have resolved in healthy children There are no commercial tests for diagnosis in the United States, but enzyme immunoassays are available in many other countries. There are a few different tests available in some research and reference laboratories; the reverse transcription–polymerase chain reaction assay is the most sensitive.21 Adenovirus is well known for causing infections of the respiratory tract along with pharyngitis, otitis media, and pharyngoconjunctival fever. Enteric adenovirus serotypes cause gastroenteritis. These strains are transmitted through the fecal-oral route. Enteric disease occurs throughout the year and affects children younger than 4 years more commonly. The incubation period is 3 to 10 days. It is most contagious during the first few days of the acute illness, but asymptomatic shedding of the virus for months is not uncommon.22 Salmonella infections usually are divided into those caused by nontyphoidal Salmonella and Salmonella typhi (typhoid fever). Nontyphoidal Salmonella account for more than 98% of the cases in the United States. Infection can result in an asymptomatic carrier state, acute gastroenteritis, bacteremia, and a disseminated abscess syndrome. It is thought that salmonellae invade the mucosa of the distal small intestine as well as the colon and produce a cholera-like enterotoxin and a cytotoxin. It is an illness marked by diarrhea, abdominal cramps, nausea, and fever; it may be manifested as dysentery or a cholera-like illness. Acute gastroenteritis occurs at any age but is most common in the first 4 years of life. Sustained or intermittent bacteremia can occur, and focal infections are seen in up to 10% of patients with Salmonella bacteremia. Animal reservoirs include poultry, livestock, and reptiles, which may be kept as pets by young children. Transmission is usually through foods such as poultry, beef, eggs, and dairy products. Other modes of transmission include ingestion of contaminated water and contact with infected reptiles, amphibians, and possibly rodents. The incubation period for gastroenteritis is 12 to 36 hours (range, 6-72 hours). Invasive disease and mortality are higher for infants and those with immunosuppressive conditions, hemoglobinopathies (e.g., sickle cell disease), malignant neoplasms, and human immunodeficiency virus (HIV) infection.23 Although it is uncommon, Salmonella serotype typhi can cause a bacteremic illness often referred to as enteric or typhoid fever. S. typhi is found only in humans, and infection implies direct contact with an infected person or with an item contaminated by a carrier. It is uncommon in the United States (approximately 400 cases per year) but is endemic in many countries. Consequently, typhoid fever infections in people in the United States usually are acquired during international travel. There is a gradual onset of symptoms that include fever, headache, malaise, anorexia, lethargy, abdominal pain, and tenderness. Patients may have hepatosplenomegaly, rose spots, and a change in mental status. It may appear as a nonspecific febrile illness in young children, in whom sustained or intermittent bacteremia may occur. Constipation is often seen early in the course of the disease, but diarrhea does occur in children.23 Treatment of nontyphoidal Salmonella infection is usually supportive. Antibiotics given to patients with nontyphoidal Salmonella infections have been found not only to be ineffective in shortening the duration of symptoms but also to prolong the carrier state. Therefore, antibiotics are generally not recommended for asymptomatic cases or for uncomplicated cases. Antibiotic treatment is indicated in infants younger than 3 months or those with complications (such as failure to improve within 5 to 7 days; bacteremia; focal infection in the central nervous system, bone, joint, kidney, or pericardium; and immunosuppressive conditions, hemoglobinopathies, malignant neoplasms, HIV infection, or chronic gastrointestinal disease). If treatment is necessary, ampicillin, amoxicillin, or trimethoprim-sulfamethoxazole usually is effective. Because of changing resistance patterns, susceptibility testing should be performed on all isolates. In areas where resistance to these antibiotics is common, ceftriaxone, cefotaxime, azithromycin, and fluoroquinolones are usually effective (fluoroquinolones are not recommended in people younger than 18 years) (Table 173-4). Table 173-4 Diarrheal Pathogens in Children and Specific Therapy Data from Pickering LK, Baker CJ, Long SS (eds): Red Book: 2009 Report of the Committee on Infectious Diseases, 28th ed. Elk Grove Village, Ill, American Academy of Pediatrics, 2009; and Custer JW, Rau RE (eds): The Harriet Lane Handbook: A Manual for Pediatric House Officers, 18th ed. Philadelphia, Mosby–Year Book, 2009. For children with S. typhi infection, antibiotics are recommended. Multidrug-resistant isolates of S. typhi are common, often requiring empirical treatment with an antibiotic such as an expanded-spectrum cephalosporin, azithromycin, or fluoroquinolone. Relapse of enteric fever occurs in up to 15% of patients and requires re-treatment. Treatment failures have occurred in people treated with cephalosporins, aminoglycosides, and furazolidone despite in vitro testing indicating susceptibility.23 Shigella species consist of four antigenic groups of 40 serotypes. Among Shigella isolates reported in industrialized nations, including the United States, approximately 86% are Shigella sonnei, 12% are Shigella flexneri, 3% are Shigella boydii, and less than 1% are Shigella dysenteriae.24 S. sonnei is the most common cause of dysentery (diarrhea with significant blood, pus, and mucus) in the United States. Shigellosis usually begins as an enterotoxin-like secretory diarrhea with watery stools and fever that may progress to bacillary dysentery with or without systemic manifestations. Clinical illness varies from mild to severe, with some patients exhibiting abdominal cramps and tenderness. Shigellosis rarely infects infants younger than 3 months and is most common between 2 and 3 years of age. Symptoms usually are self-limited and resolve within 72 hours. Extraintestinal symptoms and signs are relatively common in children with Shigella infection and may include hallucinations, confusion, and seizures. Reactive arthritis can occur weeks after the infection. Rare complications of Shigella infection include bacteremia, hemolytic-uremic syndrome (HUS), and encephalopathy (Ekiri syndrome). Ingestion of as little as 10 to 200 organisms is all that is needed for infection to occur. Transmission occurs through the fecal-oral route, contact with contaminated objects, ingestion of contaminated food or water, and sexual contact. Children 5 years and younger in daycare settings, their caregivers, and other people living in crowded conditions are at increased risk for infection. Travel to developing countries with inadequate sanitation also increases the traveler’s risk for infection. Houseflies may also be vectors through transport of infected feces. The incubation period varies from 1 to 7 days. With or without antibiotics, the carrier state usually lasts about 1 week from the onset of symptoms; chronic carrier state is rare. Antibiotics are reserved for patients with prolonged symptoms, dysentery, or underlying immune compromise.25 For this high-risk population of patients, if Shigella is suspected (patient with contact with a person with Shigella or a known regional outbreak), it is recommended that empirical treatment be started while culture and susceptibility results are awaited. According to the CDC surveillance data from 2000 to 2009, approximately 40 to 60% of isolates were resistant to ampicillin, approximately 30% were resistant to trimethoprim-sulfamethoxazole, and less than 1% were resistant to ceftriaxone and ciprofloxacin.24 Therefore, parenteral ceftriaxone or an oral fluoroquinolone (such as ciprofloxacin or ofloxacin) could be used for 5 days in adult patients who are seriously ill. For less ill adult patients, an oral fluoroquinolone is recommended. In children, parenteral ceftriaxone for seriously ill children or oral azithromycin for less ill children is recommended. Therapy is usually recommended for 5 days. A 2-day course of ceftriaxone may be used if there is a good clinical response and no extraintestinal infection25 (see Table 173-4). Campylobacter species cause a significant proportion of diarrheal disease worldwide, with 2.4 million cases yearly in the United States. According to data from the CDC, there has been a 30% decline in the incidence of infection since 1996.26 Children younger than 5 years have the highest rate of infection. It takes as few as 500 Campylobacter organisms to cause infection in exposed people. The organism is found in the gastrointestinal tracts and feces of fowl, farm animals, and pets. Of the five types, C. jejuni and C. coli are the most common. Illness consists of abdominal cramps, diarrhea, chills, fever, and Shigella-like dysentery. The clinical presentation may be similar to acute appendicitis or intussusception. Invasion of the mucosa with toxin production has been described. A 1- to 7-day incubation period is normal, and the illness usually lasts less than a week. However, approximately 20% will have a relapse or a prolonged or severe illness. Severe or prolonged disease can mimic inflammatory bowel disease. Campylobacter organisms are transmitted by ingestion of contaminated food (improperly cooked poultry and unpasteurized milk) or untreated water. Fecal-oral spread can occur, especially among very young children with diarrhea. There have been outbreaks in childcare centers, but this is rare. There has also been spread by neonates born to infected mothers that has resulted in outbreaks in nurseries. Excretion typically lasts 2 to 3 weeks without treatment. Diagnosis is made by darkfield microscopy. Oral azithromycin or erythromycin shortens the course of the illness and excretion of organisms and prevents relapse when given early (see Table 173-4). Treatment will usually eradicate the organism from the stool within 2 to 3 days. However, most children will recover without treatment.27 Y. enterocolitica is a relatively uncommon cause of simple self-limited diarrhea and vomiting in the United States. According to the CDC, the mean annual incidence is 0.3 per 100,000 people. However, for children younger than 5 years, the incidence is 1.9 per 100,000.26 Infection usually is manifested with fevers and diarrhea, which may be watery, contain mucus or blood, or both. As many as 6% of older children and adults may present with an appendicitis-like illness with right lower quadrant tenderness, usually as a result of reactive mesenteric adenitis.28 Infections usually result from eating undercooked pork or drinking unpasteurized milk. Symptoms may be prolonged, lasting 14 days or more. There have been no clinical benefits of antimicrobial therapy in the immunocompetent host with enterocolitis or mesenteric adenitis. Antibiotics are indicated for the immunocompromised with enterocolitis and in cases of septicemia and extraintestinal infections. First-line treatment of Y. enterocolitica infection is trimethoprim-sulfamethoxazole and aminoglycosides. Other effective antibiotics include cefotaxime, fluoroquinolones (patients 18 years or older), tetracycline, and doxycycline (patients 8 years of age or older). Isolates are often resistant to first-generation cephalosporins and most penicillins (see Table 173-4).29 C. difficile causes a spectrum of illnesses ranging from asymptomatic to watery diarrhea to pseudomembranous colitis. Patients usually present with diarrhea, abdominal cramps, and fever. Other common features include abdominal tenderness to palpation and dysenteric stools. Complications can include toxic megacolon and intestinal perforation. Severe disease is more common in neutropenic patients with leukemia, in infants with Hirschsprung’s disease, and in patients with inflammatory bowel disease. C. difficile gastroenteritis most often occurs in hospitalized patients, with onset during hospitalization or within 60 days after antibiotic therapy. The organism is transmitted by fecal-oral contamination. Asymptomatic infants can be colonized with the organism; intestinal colonization in healthy neonates and young infants can be as high as 50% but usually is less than 5% in children older than 2 years. The disease is thought to be brought on by the change in the gut flora as a result of antibiotic administration. Incubation time is unknown. Pseudomembranes and friable rectal mucosa are characteristic. C. difficile toxin in the stool is diagnostic. In many institutions the fecal enzyme immunoassay is used for detection of toxins A and B. The results of this test are often available within hours. The sensitivity of this test is approximately 75%. Toxigenic stool culture is the most sensitive test but takes 2 to 3 days for results. Stopping the offending agent and adding therapy with oral or intravenous metronidazole or oral vancomycin for 10 days are indicated (see Table 173-4). Up to 25% of patients experience a relapse after discontinuation of therapy, but the infection usually responds to a second course with the same agent. Drugs that decrease intestinal motility should not be given.30 Ingested C. perfringens organisms produce an enterotoxin during sporulation in the gut that causes fluid collection in ileal loops and diarrhea. The result is a short-lived (usually 24 hours) illness characterized by watery diarrhea, moderate to severe abdominal cramps, and midepigastric pain. Vomiting and fever are uncommon. Food source contamination, often from catered food services (raw meat and poultry, gravies, and dried or precooked foods), is the usual source of outbreaks. The illness cannot be transferred from person to person by the fecal-oral route. The incubation time is 6 to 24 hours. The finding of high spore counts in the stool can make the diagnosis. No specific treatment is required.31 S. aureus produces the “typical” food poisoning from ingestion of preformed enterotoxin, usually from contaminated food. Onset of symptoms is within minutes to hours of exposure. The illness is short-lived (1-2 days) and self-limited. Abrupt and sometimes violent onset of severe nausea, vomiting, abdominal cramps, and diarrhea without fever is typical. However, low-grade fever or mild hypothermia may occur. Recovery of large numbers of bacteria or enterotoxin from stool or vomitus supports the diagnosis. Treatment is supportive. No antibiotics are indicated as the disease is self-limited.32 V. cholerae is an Asian-African organism that also is seen in South America. Most cases occur in travelers returning from endemic areas. A unique strain is endemic to the Gulf Coast of the United States. The disease is acquired through ingestion of contaminated water and food, such as undercooked shellfish and raw vegetables. Because a large inoculum is required, person-to-person transmission does not occur. Diarrhea is caused by a heat-labile enterotoxin that increases cAMP through adenylate cyclase, resulting in inhibition of sodium reabsorption with chloride and fluid secretion into the gut. The illness is characterized by the painless production of large amounts of watery diarrhea without abdominal cramps or fever. Dehydration, hypokalemia, metabolic acidosis, and occasionally hypovolemic shock can occur within 4 to 12 hours if fluid losses are not replaced. Antibiotic treatment should be considered for patients with moderate to severe disease—oral doxycycline as a single dose or tetracycline for 3 days in severe cholera infection. Although it is not recommended in children younger than 8 years, the benefits may outweigh the risk of staining developing teeth. It has been shown that one course of doxycycline is unlikely to cause significant tooth discoloration. Susceptibility testing is recommended because of changing resistance patterns.33 V. parahaemolyticus is commonly found in seawater, shellfish, and fish. Illness is most commonly associated with ingestion of contaminated raw or undercooked seafood. Diarrhea, abdominal cramps, and nausea are common, whereas vomiting, headache, fever, and chills are less common. The disease usually is self-limited and does not require treatment with antimicrobials.33 E. coli is part of the normal flora in the lower gastrointestinal tract. Several types within this species are recognized to cause disease. Transmission of most diarrhea caused by E. coli is from food or water contaminated with human or animal feces or from infected symptomatic people or carriers. E. coli is identified by distinct groups of either somatic or flagellar antigens that determine virulence properties. The enterotoxigenic E. coli (ETEC) strain produces heat-stable and heat-labile enterotoxins that affect the small intestine and cause a secretory diarrhea. It is common in infants in developing countries and in travelers of all ages. It is uncommon as a cause of diarrhea in the United States. The enteroinvasive E. coli (EIEC) strain is closely related antigenically and biochemically to Shigella species and can cause a similar dysenteric illness. It invades the large bowel epithelial cells, producing enterotoxins and colonic epithelial cell death. It can cause bloody or nonbloody diarrhea and fever in all ages. The enteropathogenic E. coli (EPEC) strain is responsible for sporadic and endemic diarrhea. The diarrhea is usually watery and can be severe. The illness occurs predominantly in children younger than 2 years and mainly in developing countries. It can become chronic and cause growth retardation. This form does not produce toxins. The enteroaggregative E. coli (EAEC) strain causes watery diarrhea in people of all ages in developing and developed countries. It has been associated with a prolonged course. The enterohemorrhagic E. coli (EHEC) strain, also known as Shiga toxin–producing E. coli (STEC), produces bloody diarrhea without fever; E. coli O157:H7 is the prototype and most virulent of the EHEC. Outbreaks have been linked to ground beef, exposure to animals in public settings (petting zoos), contaminated apple cider, raw fruits and vegetables, and ingestion of water in recreational areas. The infectious dose is low, and person-to-person transmission is common during outbreaks.34 HUS is a serious sequel of EHEC infection.35 HUS consists of the triad of microangiopathic hemolytic anemia, thrombocytopenia, and renal insufficiency. It typically develops in the second week of illness, often after the diarrhea has resolved. Patients often present with pallor, weakness, irritability, and oliguria or anuria. HUS occurs in up to 20% of children with E. coli O157:H7.36 Approximately 50% of patients who have HUS will require dialysis, and 3 to 5% die. Patients with hemorrhagic colitis should be aggressively hydrated, admitted, and monitored closely (including complete blood cell count with smear and blood urea nitrogen [BUN] and creatinine concentrations) to detect changes suggestive of HUS. If patients have no laboratory evidence of hemolysis, thrombocytopenia, or nephropathy 3 days after resolution of diarrhea, their risk for development of HUS is low.35 Controversy exists about the indications for antibiotic treatment of E. coli diarrhea. Early data indicated that antimicrobials offer no substantial benefit and may increase the risk for development of HUS.37 In addition, in vitro studies have shown that subinhibitory antibiotic concentrations can increase toxin production.38 However, a subsequent meta-analysis failed to confirm the association between the use of antibiotics and the increased risk for HUS.39 In the absence of conclusive evidence, empirical antibiotics should not be administered because of the potential risk of HUS. For severe watery diarrhea in a traveler to a developing country, azithromycin or a fluoroquinolone may be considered in an older child (>18 years).34
Infectious Diarrheal Disease and Dehydration
Acute Infectious Diarrhea
Epidemiology
Principles of Disease
ETIOLOGIC CATEGORY
CLINICAL SYNDROMES
Central nervous system
Infections, space-occupying lesion
Gastrointestinal
Obstruction, peritonitis, hepatitis, liver failure, appendicitis, pyloric stenosis, midgut volvulus, intussusception, inborn errors of metabolism
Drug
Ingestion, overdose, drug effect
Endocrine
Addisonian crisis, diabetic ketoacidosis, congenital adrenal hyperplasia
Renal
Urinary tract infection, pyelonephritis, renal failure, renal tubular acidosis
Cardiac
Congestive heart failure of any cause
Infection
Pneumonia, acute otitis media, sinusitis, sepsis
Other
Psychogenic, respiratory insufficiency
ETIOLOGIC CATEGORY
CLINICAL SYNDROMES
Gastrointestinal
Malabsorption (e.g., milk intolerance, excessive fruit juice), intussusception, inflammatory bowel disease, irritable bowel syndrome, short gut syndrome
Drug
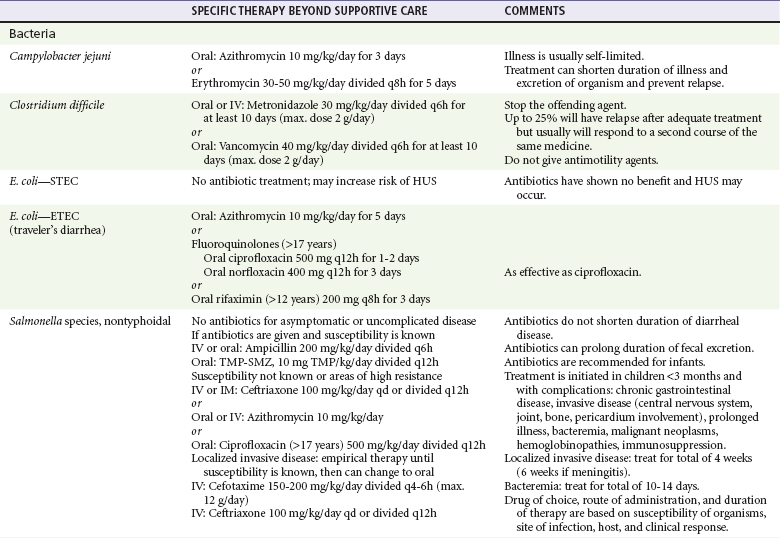
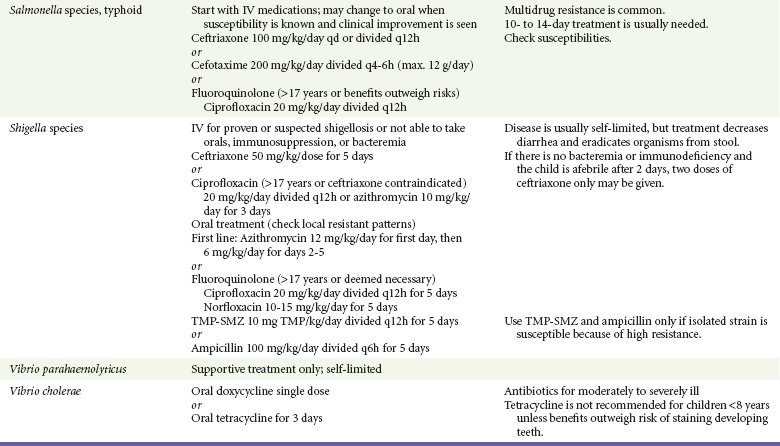
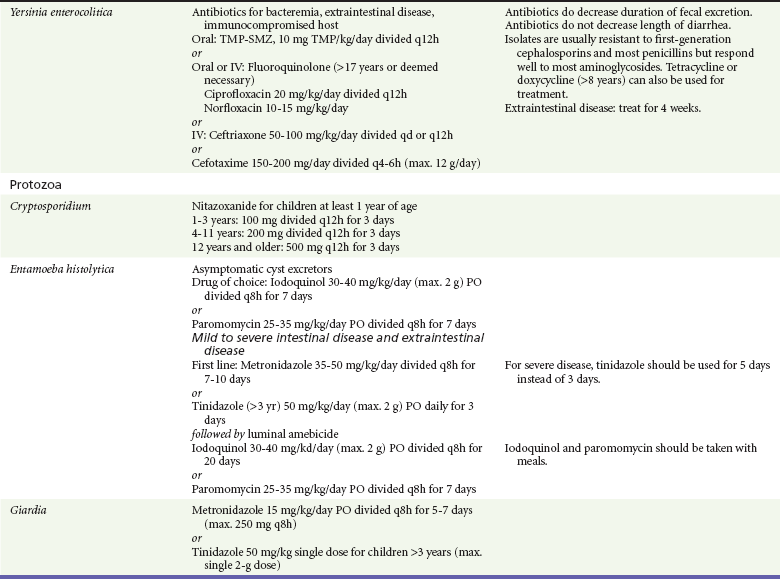
Ingestion, overdose, drug effect
Endocrine
Thyrotoxicosis, addisonian crisis, diabetic enteropathy, congenital adrenal hyperplasia
Renal
Urinary tract infection, pyelonephritis
Infection
Pneumonia, acute otitis media, sinusitis, sepsis
Other
Parental anxiety, chronic nonspecific diarrhea
Etiology
Viruses
Bacteria

Full access? Get Clinical Tree


Infectious Diarrheal Disease and Dehydration
Only gold members can continue reading. Log In or Register to continue




