Impact of the Headache on the Individual and Family
Carl G. H. Dahlöf
Glen D. Solomon
Headache is a heterogeneous condition that varies widely with respect to global severity and severity of individual attacks. Recent efforts have focused on improving the diagnostic criteria for classifying headache (4,22), but less effort has been directed toward developing reliable, valid, and clinically useful methods for assessing the impact or severity of headache on patients. Most work has primarily been focused on migraine and chronic headaches.
Migraine is a highly prevalent episodic chronic headache disease, which typically affects the sufferers during their most productive years (12,29,30,36,45). During an attack, people with severe migraine are almost completely incapacitated by a throbbing headache; nausea, vomiting, or both; and increased sensitivity to light and sound. They try to alleviate these symptoms by taking various drugs early in the attack. Very rarely, the migraineur allows the attack to take its course without treatment. Migraine is debilitating because it obstructs family obligations and social plans, results in absenteeism from work, impairs the ability to perform normal tasks at home, school, or in the workplace, produces suffering and emotional stress, and impairs health-related quality of life (HRQOL) (13,26,31,36,42,47). For that reason, migraine places a heavy economic burden on both the individual and society.
In a report issued by the World Health Organization (WHO), migraine is ranked number 12 among women and 19 in the population for degree of handicap (63). In attempts to rank the severity of different diseases, migraine has been ranked among those causing the greatest degree of handicap, together with conditions like quadriplegia, dementia, and active psychosis (34,39,40). This again clearly shows how serious migraine is and how much it affects sufferers’ everyday life, particularly bearing in mind that migraine affects the individual intermittently without apparent permanent injury and because mortality, as far as is known, among migraineurs is not higher than in the general population (41).
MEASURING IMPACT OF HEADACHE
Measurement of migraineurs’ HRQOL and disability should be taken as a multidimensional concept (Fig. 4-1). A generally applicable definition of HRQOL includes both subjective perception of one’s life situation and objectively quantifiable health factors (8,14). Accordingly, physical and social functioning as well as emotional and mental health status are very important issues to the individual (Fig. 4-1).
A population-based sample of migraine sufferers in Sweden (N = 423) was asked to rank what they value most in life by choosing from 3 of 10 alternatives. At the top of the ranking list were family life, work performance, good economy, and leisure activities/meaningful time off, which were reported by 65%, 40%, 33%, and 29%, respectively (26). The level impact of migraine on their favorite activities is demonstrated in Figure 4-2.
Assessment of Disability
The impact of migraine disability is usually measured through self-administered questionnaires. An ideal questionnaire has to be reliable, valid, and short (completed within 5 minutes). The questionnaire has to measure individual patients at all levels of severity (from mild to severe impact), enable comparisons of scores across questionnaires, and have the sensitivity to track changes over time. There are a number of validated instruments that have been developed to quantify disability: the Migraine-Specific Quality of Life Questionnaire (25), the Subjective Symptom Assessment Profile (SSAP) (15), the Minor Symptoms Evaluation Profile (MSEP) (7), the Short-Form 36 (SF-36) (37,38,42,61), the Headache Disability Inventory (23,24), the Headache Impact Questionnaire (HImQ) (54,55), Migraine Disability Assessment Questionnaire (MIDAS) (51, 52, 53), the Headache Impact Test (HIT) (2,60),
and the Migraine Attack Severity Scale (17,18), which use different distinctive approaches to measurement. Principal differences among questionnaires are reflected in their methods of administration, which can be anything from Internet/computerized, to paper-based self-administered evaluations. With respect to recall periods, they can differ from the first 24 hours of the migraine attack to consider the last 1- to 3-month period with migraine attacks.
and the Migraine Attack Severity Scale (17,18), which use different distinctive approaches to measurement. Principal differences among questionnaires are reflected in their methods of administration, which can be anything from Internet/computerized, to paper-based self-administered evaluations. With respect to recall periods, they can differ from the first 24 hours of the migraine attack to consider the last 1- to 3-month period with migraine attacks.
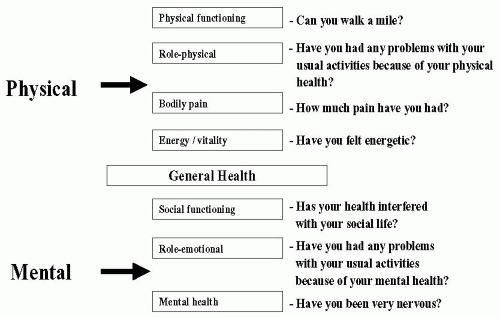 FIGURE 4-1. Chart of multidimensional concept approach to quality of life and migraine patients’ disability. |
Because of the definition of HRQOL used or the aspects of disability we are interested in, these instruments can be focused to patient’s emotional well-being, headache severity, and ability to cope with headaches or work productivity. Some of these assessment tools have the restriction of disability meaning minutes, hours, or days during which work, school, home activities were missed or affected by 50% or more (MIDAS and HImQ). Although restriction of activities from a time perspective has high face validity, research in other therapeutic areas has suggested that it may be a challenge for patients to accurately recall time missed after 2 to 4 weeks. In addition, some of the currently available assessment tools are not likely to demonstrate changes over time because of different migraine interventions. Indeed, the full impact of migraine is not easy to measure, although some instruments have been developed to quantify migraine disability and improve communication between patients and healthcare professionals.
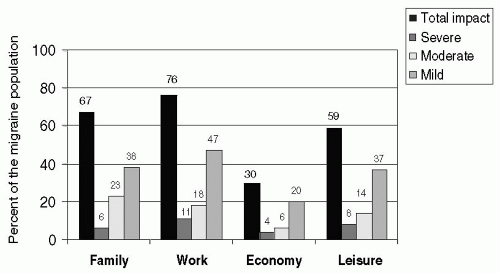 FIGURE 4-2. The impact of migraine on the favorite activities family life, work performance, good economy, and leisure in a population-based sample of migraine sufferers in Sweden (N = 422) (26). |
Almost all, if not all, migraineurs take medications, whether nonprescription or prescription, in an attempt to rapidly relieve the most debilitating symptoms of the migraine attack—pain, nausea, phono- and photophobia (9,26,30,35). The success of medications and other treatments dictates the extent of the sufferer’s immediate disability, which may range from beginning to resume activities within hours to being immobilized in bed for days, arising only with the urge to vomit. Despite of treatment used, total recovery still seems to follow the natural duration of the attack. We developed a questionnaire for measuring disability and patients’ quality of life during the migraine attack, namely, the Minor Symptoms Evaluation Profile-Acute (MSEP-Acute) (Fig. 4-2) (11). Figure 4-2 (left) clearly shows the difference between patients’ answers in the MSEP-Acute questionnaire done between and during migraine attack, when the answers were left shifted
at baseline and right shifted toward “deterioration” during the attack. Although placebo did not change these results (middle), sumatriptan 8-mg subcutaneous injection caused an improvement and shifted the answers toward baseline values obtained outside the migraine attacks (see Fig. 4-2).
at baseline and right shifted toward “deterioration” during the attack. Although placebo did not change these results (middle), sumatriptan 8-mg subcutaneous injection caused an improvement and shifted the answers toward baseline values obtained outside the migraine attacks (see Fig. 4-2).
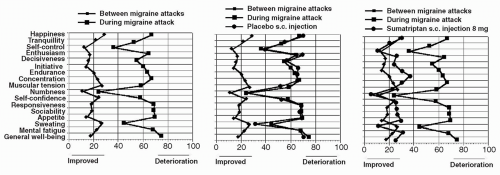 FIGURE 4-3. The MSEP-acute assessments before and after acute migraine treatment with sumatriptan 8-mg subcutaneous injection and placebo (11). |
Another illustrative example for using the self-administered standardized questionnaires is the SSAP test, developed for general well-being evaluation of migraine patients and other patient categories (Fig. 4-3). In Figure 4-3, through the SSAP diagram, it can be demonstrated that the area of symptoms between migraineurs without migraine attack is larger than that of age and gender-matched controls. From this evaluation it appears that migraine affects the symptom profile of the migraineurs also during days when they are not suffering attacks. Thus, in addition to the disability perceived during the migraine attack, it seems that some impairment is also experienced between the attacks (6,10,27). The unpredictability of migraine and anxiety about future attacks often thus has an interictal influence. When population-based sample of migraineurs were asked about recovery, 43%, 43%, and 9%, respectively (4% no response), stated that they recovered “completely,” “more or less” and “not at all” between the attacks (26). In other words, less than half recovered fully between the attacks.
Moreover, there are other questionnaires, like the SF-36, which by evaluating eight different dimensions, enable us to compare quality of life in migraineurs with that of patients with other diseases. Subjects (n = 845) were surveyed 2 to 6 months after participation in a placebo-controlled clinical trial and asked to complete a questionnaire including the SF-36 Health Survey, a migraine severity measurement scale and demographics. Results were adjusted for severity of illness and comorbidities. Scores were compared with responses to the same survey by the U.S. sample and by patients with other chronic conditions, like depression and osteoarthritis (42).
Related posts:







Full access? Get Clinical Tree


