Fig. 54.1
Schematic diagram showing the pathway of the ilioinguinal, iliohypogastric, and genitofemoral nerve. GFN genitofemoral nerve (Reproduced with permission from Philip Peng Educational Series)
The IH nerve pierces the transversus abdominis muscle above the iliac crest, midway between the iliac crest and the twelfth rib. The II nerve runs caudally and parallel to the IH nerve. Here, both nerves can be found consistently (90 %) between the transversus abdominis and internal oblique muscles [2, 3]. Terminal branches of the IH nerve perforate the external oblique muscle aponeurosis approximately 4 cm lateral to the midline to supply the skin over the lower portion of the rectus abdominis [2, 3]. The IH nerve also provides sensory innervation to the skin above the tensor fasciae latae through a lateral cutaneous branch. Terminal branches of the II nerve enter the inguinal canal through the deep inguinal ring; it may lie upon the cremaster muscle and fascial layer of the spermatic cord in men or round ligament in women [4, 5]. Here, the II nerve is often accompanied by the genital branch of the GF nerve, and wide variations in the course of these nerves within the inguinal canal have been documented [6–9]. The terminal sensory branches may innervate the skin of the mons pubis, inner thigh, inguinal crease, and anterior surface of the scrotum or anterior one third of the labia (Fig. 54.2).
Fig. 54.2
Cutaneous innervation of the ilioinguinal region (Reproduced with permission from Dr. Danilo Jankovic)
The GF nerve originates from the first and second lumbar nerve roots (Fig. 54.1). It emerges on the anterior surface of the psoas muscle either as a single trunk or separate genital and femoral branches [6]. The femoral branch passes laterally over the external iliac artery and then penetrates the fascia lata to enter the femoral sheath. Terminal branches provide cutaneous innervation to the femoral triangle [7]. The genital branch will also cross in front of the external iliac artery but then passes through the ventral aspect of the internal ring of the inguinal canal (Fig. 54.1). Anatomical studies describe this branch as running between the cremasteric and internal spermatic fascia, incorporating with the cremasteric fascia, or lying outside of the spermatic cord [5, 7, 8]. Terminal sensory branches may innervate the scrotum and possibly the upper, inner, and medial thigh [5].
However, the main concept to remember when dealing with the “border nerves” is the high rate of variability they are associated with. Anatomical studies highlight this variability, which has been reported with respect to their origin and spinal contribution [10], communication between nerves, penetration of fascial layers, branching patterns, and dominance patterns [2]; in some cases, one of the nerves may be entirely absent [9]. Although the general anatomy of the IH and II nerves has been well documented in standard anatomy textbooks, recent studies related to nerve injury during surgery or based on cadaver dissections were able to identify multiple and different spinal nerves contributing to the formation of these nerves. The II and IH nerves mainly originate from the T12 and L1 nerve roots, but a contribution from T11 to L3 exists in a minority of patients [10].
The most consistent anatomical location for the II and IH nerves to perforate the abdominal muscular layers is lateral and superior to the anterior superior iliac spine, where they run between the transversus abdominis and internal oblique muscular layers, even though the distance from the ASIS to the point the nerves enter the fascial layer can widely vary [11, 12].
As well, communication between the GF, IH, and II nerves (as well as the lateral femoral cutaneous nerve) is common and results in sensory overlap. Finally, the sites at which the II and IH nerves pierce the abdominal wall muscle layers are significantly variable [13].
Special considerations are needed for pediatric patients. Anatomically, pediatric patients have varying II and IH nerves compared with adults; anatomical results from adults cannot be downscaled to infants and children, in whom the iliohypogastric and ilioinguinal nerves lie closer to the ASIS than originally thought [14], and differences have been noted according to different age groups [15].
Existing Technique for Neural Blockade
As discussed above, there is a high degree of anatomic variability in not only the course of the nerves but also their branching patterns, areas of penetration of the fascial layers, and dominance patterns [2]. By far, the most consistent location of the II and IH nerves is lateral and superior to the ASIS, where the nerves are found between the transversus abdominis and internal oblique muscular layers in nearly 90 % of the cases [16, 17]. While most of the anatomic variations occur medial to the ASIS, virtually all landmark-guided injection techniques described in the literature are performed in the anterior abdominal wall [2, 3, 18].
Because the existing landmark-based techniques rely on blind infiltration of local anesthetic through different layers, the risk of complications are well understandable: these include inadvertent femoral nerve block [14, 19], colonic puncture [20, 21], and vascular injury [22]. Nevertheless, block failure is still an important matter of concern, and failure rate of the blind technique lies in the range of 10–40 % [14, 23]. This is attributed to the potential for injecting local anesthetics into the wrong abdominal plane [23], and in some situation, it leads to injection inside the peritoneum [24].
As well, the conventional description of the blockade of the genital branch of the GF nerve is mainly a “blind” technique [25, 26] and relies on the pubic tubercle, inguinal ligament, inguinal crease, and femoral artery as landmarks. One involves infiltration of local anesthetic immediately lateral to the pubic tubercle caudal to the inguinal ligament [25]. In another method, a needle is inserted into the inguinal canal to block the genital branch [26]. The blind techniques described are essentially infiltration techniques and rely on high volumes of local anesthetic for consistent results. Although the basis of this landmark is not clear, the needle is likely directed toward the spermatic cord, and important structures of the spermatic cord (testicular artery and vas deferens) or the peritoneum are at risk.
Ultrasound-Guided Injection Technique
Advantages of ultrasound guidance include the identification of muscular and fascial layers (including structures lying deeper to the peritoneum), the visualization of needle’s trajectory and spread of injectate, and the detection of vascular structures. Ultrasound helps physicians to overcome the wide anatomic variability associated with the structures in this area, helping to identify the nerves themselves, or the plane they lie within. Ultrasound guidance has demonstrated to improve accuracy in the injection of local anesthetics, with less risk of inadvertent injections in the wrong fascial plane [24], reduced amount of local anesthetics used for anesthesia, and lower consumption of systemic pain medications compared to landmark techniques [23, 27].
The IH and II nerves are superficial nerves, best viewed with a linear probe of high frequency (6–13 MHz). In very obese patient, a linear medium-frequency probe may be useful. Most of clinical studies or reports used ASIS as landmark, and the position of the probe was above ASIS and moved along the line joining the ASIS and umbilicus. This approach carries some limitation: when the probe is placed too near to ASIS, the external oblique muscle layer may be missed; when the probe is too far away from the ASIS (the “bone shadow of iliac crest” not in the scan), the nerve seen in between the transversus abdominis and internal oblique muscular layers is likely the 12th intercostal nerve or subcostal nerve instead.
The recommended area for ultrasound scanning of II and IH nerves is lateral and superior to the anterior superior iliac spine (Fig. 54.3), because the two nerves are detectable in this area in 90 % of the cases. The probe is placed cranial and three fingerbreadths lateral to the ASIS with the transducer perpendicular to the inguinal ligament and its lateral end in contact with the iliac crest (Fig. 54.3). At this position, the iliac crest will appear as a hyperechoic structure adjacent to which will appear the three muscular layers of the abdominal wall (Figs. 54.4 and 54.5). Below the transversus abdominis, peristaltic movements of the bowel may be detected. Once the muscular layers are identified, the II and IH nerves will be found in the split fascial plane between the internal oblique and transversus abdominis muscle layers. Both nerves should be within 1.5 cm of the iliac crest at this site, with the II nerve closer to the iliac crest [28]. The nerves are usually in close proximity to each other [9] and located on the “upsloping” split fascia close to the iliac crest. In some cases, the nerves may run approximately 1 cm apart. The deep circumflex iliac artery which is close to the two nerves in the same fascial layer can be revealed with the use of color Doppler (Fig. 54.6). A neural structure within the fascial split may also be seen medial and on the flat part of the internal oblique and transversus abdominis muscle junction: this is the subcostal nerve, and if mistaken for the II and IH nerves, the nerve blockade will result in aberrant distribution of anesthesia.
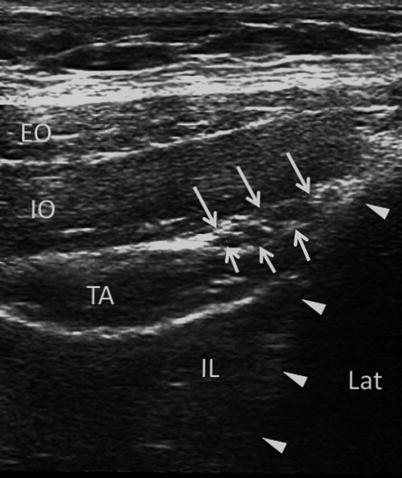
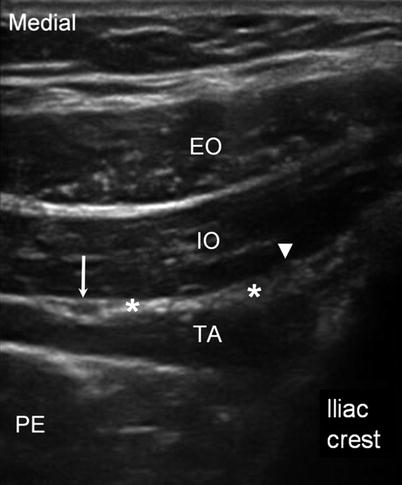
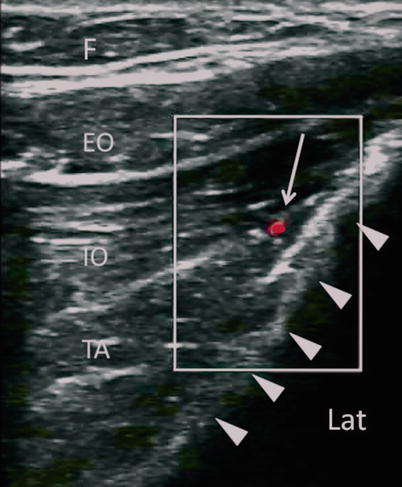
Fig. 54.3
Similar view as in Fig. 54.3. In addition to the ilioinguinal (solid arrowhead) and iliohypogastric (*) nerves, a third nerve appears and is usually mistaken as the ilioinguinal nerve but is much further from the iliac crest. It is the subcostal nerve (12th intercostal nerve) indicated by line arrow. EO external oblique muscle, IO internal oblique muscle, TA transversus abdominis muscle, PE peritoneum, (Reproduced with permission from Philip Peng Educational Series)
Fig. 54.4
Figure showing the three layers of the muscles and the fascial split (white line arrows) with the ilioinguinal and iliohypogastric nerves inside. Solid triangles outline the iliac crest. EO external oblique muscle, IO internal oblique muscle, TA transversus abdominis muscle, IL iliacus (Reproduced with permission from Philip Peng Educational Series), Lat lateral side
Fig. 54.5
Similar view as in Fig. 54.3. In addition to the ilioinguinal (solid arrowhead) iliohypogastric (*) nerves, a third nerve appears and is usually mistaken as the ilioinguinal nerve but is much further from the iliac crest. It is the subcostal nerve (12th intercostal nerve) indicated by line arrow. EO external oblique muscle, IO internal oblique muscle, TA transversus abdominis muscle, PE peritoneum (Reproduced with permission from Philip Peng Educational Series)
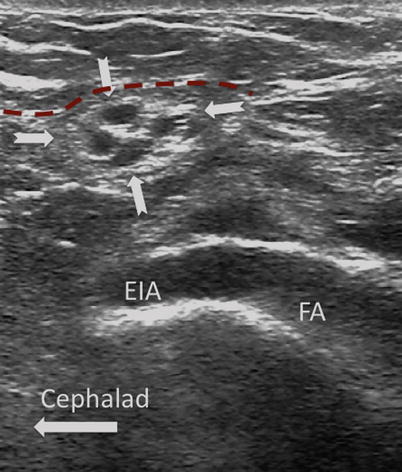
Fig. 54.6
Similar view as in Fig. 54.3 with color Doppler. A branch of the deep circumflex iliac artery is shown in red color. Solid arrows outline the iliac crest. F subcutaneous fat, EO external oblique muscle, IO internal oblique muscle, TA transversus abdominis muscle, Lat lateral (Reproduced with permission from Philip Peng Educational Series)
In some patients (those with previous surgery, multiple childbirth) or when the procedure is performed by inexperienced practitioners, either the II and IH or the fascia split is difficult to visualize; in these cases, the target will be the fascial plane between the internal oblique and transverse abdominal muscles [29].
Both out-of-plane and in-plane techniques can be used and have been described [28, 30]. As the two nerves run very closely within the fascial plane (sometimes as a common trunk) and frequently overlap in sensory innervation, a selective block of one of the two nerves has recently been demonstrated to be very difficult to realize, even in experienced hands and injecting minimal volumes of local anesthetics [31].
Ultrasound-guided blockade of the genital branch of the GF nerve has been described in several review articles [2, 3, 18, 32]. The genital branch is difficult to visualize directly unless a high-frequency probe (up to 18 MHz) is used. Furthermore, the GF nerve can be found within or outside the spermatic cord. Thus, the most reliable method is to infiltrate the inguinal canal and deposit the injectate both inside and outside the spermatic cord [2, 3]. The patient is placed in a supine position, and surface anatomy of the ASIS, inguinal ligament, and femoral artery is established. A linear ultrasound transducer of high frequency (6–13 MHz) is placed over the femoral artery along its long axis (Fig. 54.2). The transducer is moved cephalad over the artery, which starts to descend at a steep angle toward the inguinal ligament. At this point, the femoral artery transitions to become the external iliac artery and runs in a retroperitoneal plane (Fig. 54.7). Once the external iliac artery is identified, the inguinal canal can be viewed superficial to the vessel as an oval, soft tissue structure (Fig. 54.7). This will contain the spermatic cord in men and the round ligament in women. The canal is then scanned medially, so that the final ultrasound probe position is approximately one fingerbreadth away from the pubic tubercle. In males, testicular arteries may be identified in the spermatic cord as pulsatile structures and confirmed with the use of color Doppler (Fig. 54.8). Vessels may be accentuated by asking the patient to cough or perform a Valsalva maneuver, which increases blood flow through the pampiniformis plexus. The vas deferens may also be identified as a thick, tubular structure.