Key Clinical Questions
Introduction and Epidemiology
Hypertension is the most common reason for patients to seek medical attention in the United States. It affects over 70 million people in the United States, with global numbers approaching one billion. The annual costs of hypertension, both direct and indirect, are estimated to be $50 billion in the United States alone.
The most popular classification of hypertension is that of the Seventh Report of The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7). Blood pressure is classified as normal, prehypertension, stage 1 hypertension, and stage 2 hypertension (Table 252-1).
| Normal | Prehypertension | Stage I | Stage II | |
|---|---|---|---|---|
| Systolic blood pressure (in mm Hg) | < 120 | 120–139 | 140–159 | > 160 |
| Diastolic blood pressure (in mm Hg) | < 80 | 80–89 | 90–99 | > 100 |
Patients with untreated or inadequately treated hypertension are prone to sudden elevations in blood pressure and the development of hypertensive crises. Up to 1% of all hypertensive patients will have a hypertensive crisis in their lifetime. Hypertensive crises come in two forms. In a hypertensive emergency, a surge in blood pressure is accompanied by end-organ damage. Hypertensive urgency is an acute elevation in blood pressure without end-organ damage. There is no blood pressure threshold that defines a hypertensive crisis. Most patients have pressures that exceed 180/120 mm Hg, with diastolic blood pressures over 120 mm Hg being most strongly associated with end-organ damage. Patients who develop a hypertensive crisis in settings other than chronic essential hypertension may develop end-organ damage at lesser degrees of blood pressure elevation, as they lack the vascular smooth muscle hypertrophy that provides some protection against the effects of uncontrolled hypertension.
Pathophysiology
Many elements are involved in blood pressure regulation, such as the renin-angiotensin-aldosterone system (RAAS) of the kidney. Renin is released by the juxtaglomerular apparatus in response to low kidney perfusion, elevated sympathetic response, low dietary sodium, and other stimuli. Renin cleaves circulating angiotensinogen to form angiotensin I, which in turn is cleaved to angiotensin II by angiotensin-converting enzyme (ACE). Angiotensin II is a potent arteriolar constrictor that increases both systolic and diastolic blood pressure. It also signals the adrenal cortex to secrete aldosterone, which increases the reabsorption of sodium from urine, sweat, saliva, and bowel.
Catecholamines from the sympathetic nervous system greatly affect blood pressure, especially epinephrine. Binding of epinephrine to α1 receptors leads to vasoconstriction and increased peripheral vascular resistance, causing blood pressure to rise. Binding to β1 receptors increases heart rate and cardiac output, which also raises blood pressure. The endothelium also locally produces vasoactive substances that affect blood pressure, such as the vasodilators nitric oxide, prostacyclin, and bradykinin, and the vasoconstrictor endothelin-1.
Arterial baroreceptors are mechanoreceptors in the carotid sinuses and aortic arch. When blood pressure rises, the mechanoreceptors are stretched, decreasing their firing rate. This decreases central sympathetic outflow and increases parasympathetic tone, lowering blood pressure. Conversely, when blood pressure falls, decreased stretching of mechanoreceptors increases their firing rate, stimulating sympathetic and inhibiting parasympathetic outflow. This feedback loop is sensitive to acute fluctuations in blood pressure, but in chronic essential hypertension, the set point rises and a higher basal blood pressure is tolerated.
In general, hypertensive crises result from a breakdown in arterial adaptation to chronic hypertension, leading to a vicious cycle of vascular injury. The endothelium adapts to high blood pressure by smooth muscle hypertrophy and vasoconstriction. Prolonged smooth muscle contraction eventually leads to endothelial dysfunction, diminished nitric oxide production, and a failure of autoregulation. Focal vasodilation, endothelial damage, and increased vascular permeability result, with leakage and deposition of fibrinogen and plasma proteins in blood vessel walls. The coagulation cascade is activated and fibrinous clot is formed, leading to ischemia, further endothelial injury, inflammation, and release of vasoconstrictive mediators, perpetuating the cycle of injury.
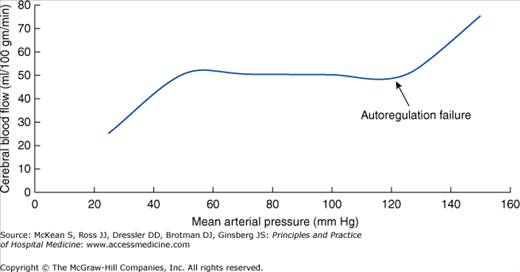
Under normal conditions, the brain autoregulates cerebral blood flow (CBF) to ensure that the high metabolic demands of neuronal cells are met, despite fluctuations in blood pressure.
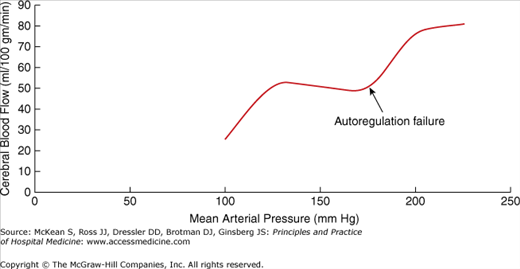
Normally, CBF is maintained at 50 mL blood per 100 g of brain tissue per minute (Strandgaard 1973) (Figures 252-1 and 252-2). The upper limit of autoregulation is a mean arterial pressure (MAP) of > 120 mm Hg for normotensive patients and > 180 mm Hg for hypertensive patients. (The higher threshold in hypertensive patients is due to vascular hypertrophy and other morphologic changes from chronic elevations in blood pressure.) If the upper limit of autoregulation is surpassed, endothelial dysfunction and damage may occur, the blood-brain barrier may break down, and cerebral edema and microhemorrhages may develop, giving rise to hypertensive encephalopathy.
The lower limit of CBF autoregulation also differs between hypertensive and normotensive patients. Hypertensive patients may show signs or symptoms of cerebral hypoxemia, including loss of consciousness, coma, or seizures, at MAP levels of 50 ± 5 mm Hg and below, whereas normotensive patients will show these symptoms at a MAP of 40 ± 5 mm Hg and below. This has important implications for the management of hypertensive emergencies: too rapid lowering of blood pressure in these patients poses a risk of cerebral hypoperfusion.
Causes
The most common causes of hypertensive crises are inadequate adherence to antihypertensive therapy and previously undiagnosed essential hypertension. Patients who stop taking some antihypertensive drugs may develop severe rebound hypertension, especially those who abruptly discontinue beta-blockers or clonidine. Chronic renal failure and sleep apnea are common medical causes of poorly controlled hypertension. Cocaine, amphetamines, phencyclidine, aminophylline, phenylephrine, diet pills, and other sympathomimetic drugs may cause hypertensive crises. Patients who take monoamine oxidase inhibitors (MAOIs), including the antibiotic linezolid and over-the-counter drugs with MAOI activity, such as St. John’s wort, are at risk for developing hypertensive crisis with confusion if they also ingest selective serotonin reuptake inhibitors, tricyclic antidepressants, meperidine, tramadol, methadone, dextromethorphan, or tyramine-containing foods such as red wine, aged cheeses, smoked or pickled meats, and avocado. Bevacizumab, a monoclonal antibody against vascular endothelial growth factor that is approved for use in several advanced adenocarcinomas, may lead to hypertensive crisis.
Although most patients with a hypertensive crisis do not have a secondary cause of hypertension, such as renal artery stenosis, acute glomerulonephritis, preeclampsia, pheochromocytoma, scleroderma renal crisis, or Cushing syndrome, an evaluation for secondary hypertension should be considered, especially in the presence of compatible signs and symptoms, as described elsewhere in this volume.
Related posts:
 Strategies for Cost-Effective Care
Strategies for Cost-Effective Care
 Building, Growing, and Managing a Hospitalist Practice
Building, Growing, and Managing a Hospitalist Practice
 Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
 Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist
Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist

Full access? Get Clinical Tree


