TOPICS
Hypertensive disorders seriously complicate approximately 2% to 8% of all pregnancies.1 Indeed, 19% of pregnancy-related maternal mortality is due to complications related to hypertensive disorders.2 Hypertensive disorders during pregnancy involve a variety of clinical entities, including gestational hypertension, preeclampsia, eclampsia, chronic hypertension, superimposed preeclampsia on chronic hypertension, and hemolysis, elevated liver enzymes, low platelets (HELLP) syndrome.3 The normal physiologic changes of pregnancy result in a net reduction of systolic, diastolic, and mean arterial blood pressure by midpregnancy because of decreased systemic vascular resistance and the presence of a low resistance to flow placenta. At the end of term pregnancy, the blood pressure returns to baseline prepregnant level.4
Gestational hypertension occurs when a pregnant woman without a previous history develops isolated hypertension (greater than 140/90 mm Hg) after 20 weeks’ gestation. It is not associated with significant proteinuria or other symptoms and signs of preeclampsia and resolves within 12 weeks’ postpartum.
Preeclampsia is diagnosed when a pregnant woman develops new onset hypertension (greater than 140/90 mm Hg) after 20 weeks’ gestation often in conjunction with proteinuria (greater than 300 mg in a 24-hour collection). In 2013, the American College of Obstetricians and Gynecologists (ACOG) updated its diagnostic criteria of preeclampsia-eclampsia and eliminated the dependence on proteinuria for diagnosis. To reflect the syndromic nature of preeclampsia, in the absence of proteinuria, it is diagnosed as hypertension in association with thrombocytopenia, impaired liver function, renal insufficiency, pulmonary edema, or cerebral or visual disturbances.5 Preeclampsia may be classified as severe based on any of the following:
• Systolic blood pressure greater than or equal to 160 mm Hg, or diastolic blood pressure greater than or equal to 110 mm Hg
• Thrombocytopenia (platelet count less than or equal to 100,000/mm3)
• Impaired liver function as indicated by elevated liver enzymes (to twice normal levels) and/or severe persistent right upper quadrant pain
• Renal insufficiency as indicated by serum creatinine concentration greater than 1.1 mg/dL or a doubling of the serum creatinine
• Pulmonary edema
• New-onset cerebral or visual disturbances
The most recent report of ACOG’s task force on hypertension in pregnancy has eliminated proteinuria greater than 5 g from the diagnostic criteria for severe preeclampsia for the reason that there is a minimal relationship between the quantity of urinary protein and pregnancy outcome.5
Eclampsia is defined by new-onset seizures or impaired mental state (ie, coma) in a preeclamptic woman. It is not a separate entity from preeclampsia but rather signifies a continuum of severity. Eclampsia carries a high maternal morbidity and mortality rate. Intracerebral hemorrhage/stroke, pulmonary aspiration, cardiopulmonary arrest, acute renal failure, and death are major complications of seizures. In addition, there is significant potential for fetal jeopardy.6
HELLP syndrome is considered a variant of preeclampsia. Aside from hemolysis, elevated liver enzymes, and low platelets, associated symptoms may include hypertension, proteinuria, right upper quadrant/epigastric pain, nausea and vomiting, and headache. Clinical presentation can be variable, and patients may initially be normotensive or without proteinuria. HELLP may devolve rapidly to various maternal complications, including disseminated intravascular coagulation (DIC), placental abruption, renal failure, and cerebral and liver hemorrhage. It is associated with a 70% preterm delivery rate. HELLP is an indication for stabilization and delivery, especially at 34 weeks’ gestation or later.7
Chronic hypertension is diagnosed when blood pressure levels are greater than or equal to 140 mm Hg systolic or greater than or equal to 90 mmHg diastolic before pregnancy or before 20 weeks’ of gestation, or when elevated blood pressures fail to resolve 12 weeks’ postpartum. The pathophysiology of chronic hypertension is much better understood than that of preeclampsia. Chronic hypertension with superimposed preeclampsia occurs when pregnant women who have a history of chronic hypertension before pregnancy develop preeclampsia. The diagnosis is made in the presence of new-onset proteinuria or a sudden increase in proteinuria and/or hypertension, or when other manifestations of severe preeclampsia appear. Maternal and perinatal morbidity is higher with superimposed preeclampsia than it is with preeclampsia alone.
The goal of classifying hypertensive disorders during pregnancy by blood pressure, proteinuria, seizures, and organ system involvement is to allow management decisions to be made about the timing of delivery and the initiation of therapies. The only definitive treatment of preeclampsia is delivery of the neonate and placenta.
PREECLAMPSIA
Preeclampsia is a leading cause of maternal and perinatal morbidity and mortality. Even in developed countries with low maternal mortality rates, preeclampsia/eclampsia remains a leading cause of maternal morbidity and mortality.1 Maternal complications from hypertensive disorders include placental abruption, eclampsia, cerebrovascular accidents, multisystem organ failure, and DIC. Maternal deaths are due mostly to intracranial hemorrhage, cerebral infarction, acute pulmonary edema, and hepatic rupture or failure. Preeclampsia also results in fetal complications such as preterm birth, intrauterine growth retardation, and fetal/neonatal death.8
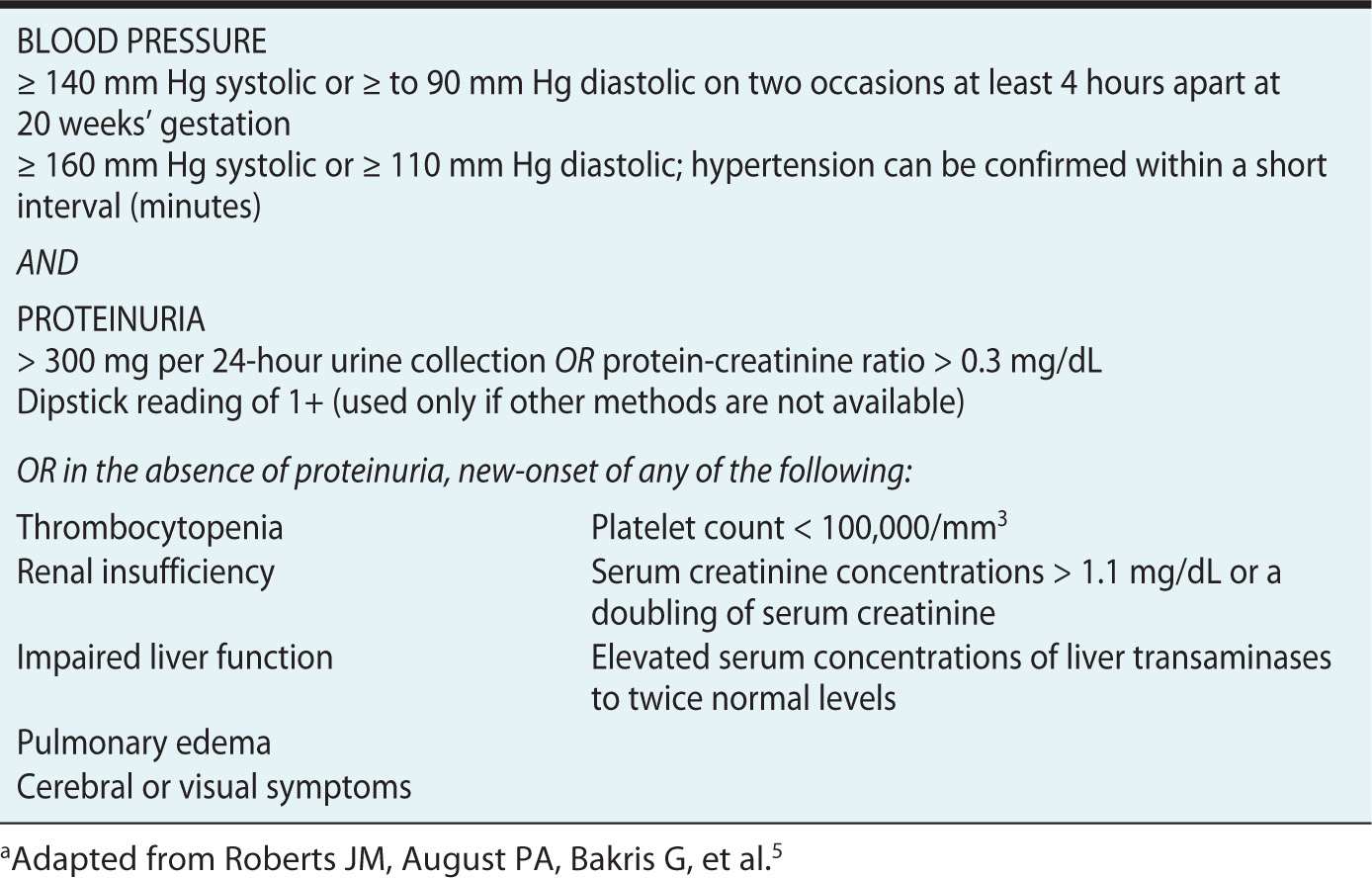
Preeclampsia is a multisystem disease that is typically diagnosed when new-onset hypertension occurs with proteinuria after 20 weeks’ gestation (Table 22-1). Preeclampsia can evolve during its course, and complications could be avoided if clinicians stay vigilant for the progression of the disease. Diagnosis and interventions are sometimes delayed because of the absence of proteinuria.5 Some women may have an atypical presentation of preeclampsia, where signs and symptoms may vary and would not fit into the classical definition. Atypical preeclampsia can present before 20 weeks’ gestation, without proteinuria, or as proteinuria only.9 Edema was previously a part of the diagnostic criteria but has been excluded because edema is a common physical finding in many pregnant women and is therefore nonspecific. Preeclampsia usually presents near term or during the intrapartum period. It can also manifest in the postpartum period, usually within 7 days postdelivery. Risk factors include nulliparity, age greater than 40 years, obesity, previous preeclampsia, multiple gestation, diabetes mellitus, preexisting kidney disease or chronic hypertension, sickle cell disease, and in vitro fertilization (possibility of multiple pregnancies).
Table 22-1. Criteria for Diagnosis of Preeclampsiaa
Depending on the time of presentation, preeclampsia is classified into early-onset (develops before 34 weeks’ gestation) and late-onset (develops at or after 34 weeks’ gestation) types. Women with early-onset disease usually develop more severe disease.10 Severe preeclampsia, characterized by blood pressure greater than 140/90 mm Hg and proteinuria greater than 5 g/24 hours, is associated with a higher maternal morbidity and mortality because patients are at higher risk for HELLP syndrome, DIC, cerebrovascular accidents, pulmonary edema, renal failure, placental abruption, and eclampsia than women with mild preeclampsia.
Serum uric acid levels are often elevated early in the disease process, and this has been used as a sentinel marker of the disease. However, hyperuricemia has poor correlation with severity of disease and maternal/fetal complications.11
HELLP Syndrome
HELLP syndrome complicates 10% to 20% of cases of severe preeclampsia. The diagnostic criteria of HELLP syndrome include hemolysis with elevated serum lactate dehydrogenase level (greater than 600 IU/L), increased serum aspartate aminotransferase level (greater than 70 IU/L), and decreased platelet count (less than 100,000/mm3). Hemolysis is defined as the presence of microangiopathic hemolytic anemia and is confirmed by visualizing Burr cells (contracted red blood cells with spikes) and schizocytes (fragmented) on a peripheral blood smear.7
Eclampsia
Eclampsia is the occurrence of seizures and/or coma in a patient with preeclampsia. In the United States, the incidence of eclampsia is relatively low, ranging from 0.03% to 0.7%. Eclamptic seizures are of tonic-clonic type and in majority of patients, convulsions appear during the antepartum period. Eclamptic convulsion also may appear during the postpartum period, within 7 days after delivery of the infant. Associated neurologic complications in patients with eclampsia include cortical blindness, aphasia, hemiparesis, facial nerve palsy, postpartum psychosis, and cerebrovascular accidents. Unlike hypertensive encephalopathy, focal neurologic deficits and papilledema are not commonly noted in eclampsia.12
Management of eclamptic seizure includes termination of the convulsion, protection and maintenance of the airway, adequate oxygenation, establishment of intravenous access, and monitoring of fetal well-being.
Pathophysiology of Preeclampsia
The placenta is the pathogenic focus of preeclampsia. The exact mechanism in which the abnormal placenta leads to multisystem effects which characterize preeclampsia is not well understood. Currently, the most widely accepted theory is that the placenta fails to embed adequately into the myometrium, which leads to poor placental perfusion. As a consequence, the placenta becomes hypoxic and releases factors into the circulation that damage the maternal endothelium and give rise to the multisystem effects of preeclampsia. In normal pregnancy, the villous cytotrophoblast invades the inner third of the myometrium, and the spiral arteries lose their endothelium and most of their muscle fibers. The spiral arteries are then structurally modified into low-resistance vessels that are unresponsive to vasoactive stimuli. In preeclampsia, there is defective invasion of the spiral arteries by the cytotrophoblast and impaired spiral artery remodeling, which results in abnormal placentation and development of high-resistance vessels that are hyperresponsive to vasomotor stimuli. Increased uterine arterial resistance leads to decreased placental perfusion and placental infarcts. This chronic placental ischemia causes fetal intrauterine growth restriction. In addition, substances such as free radicals, oxidized lipids, cytokines, and endothelial growth factors may be released into the maternal circulation in response to the chronic hypoxia, which create widespread maternal endothelial dysfunction. Necrotic injury of syncytiotrophoblast due to placental hypoxia releases antiangiogenic factors, such as soluble form of the vascular endothelial growth factor receptor and soluble endoglin. Normal endothelium is responsible for preventing platelet activation, keeping fluid in the intravascular compartment, and buffering the response to pressors. In preeclampsia, the endothelium becomes hyperpermeable and thrombogenic, and vascular tone is increased.13,14
Clinical Manifestations of Preeclampsia
Manifestations of severe preeclampsia occur in all organ systems as a result of widespread endothelial dysfunction.
CENTRAL NERVOUS SYSTEM
Central nervous system (CNS) symptoms of preeclampsia/eclampsia include severe persistent headaches, visual disturbances, hyperreflexia, seizures, and coma. CNS manifestations are a result of loss of cerebral autoregulation. Breakdown of autoregulation and disruption of the blood-brain barrier due to a rapid rise in blood pressure and forced dilation of the cerebral vessels may result in cerebral edema, similar to the changes seen in hypertensive encephalopathy.15 Eclampsia, which is defined as new-onset seizures during pregnancy, most commonly occurs in the intrapartum period or within 48 hours of delivery.
PULMONARY
Preeclampsia is reported to be one of the important causes of pulmonary edema in pregnant women. Endothelial injury, combined with decreased colloid osmotic pressure, is the primary underlying mechanism for increased leakage of intravascular fluid into the lungs.16
CARDIOVASCULAR
The physiologic changes in the cardiovascular system during normal pregnancy involve a state of high cardiac output, primarily due to increased stroke volume, and decreased systemic vascular resistance. However, in patients with preeclampsia, changes in the cardiovascular system reverse to a state of low cardiac output with high systemic vascular resistance. However, myocardial contractility remains unaffected.17 Increased vascular tone and sensitivity in preeclampsia is responsible for these changes, manifested by hypertension, vasospasm, and end-organ ischemia. Sustained increases in blood pressure and systemic vascular resistance can dramatically reduce intravascular volume with severe disease. Acute elevations in blood pressure, especially if severe, may render the patient at risk for hypertensive encephalopathy, cerebrovascular hemorrhage, myocardial ischemia, and congestive heart failure.
HEMATOLOGIC
Related posts:







Full access? Get Clinical Tree


