Hypertension, Obesity, Type II Diabetes Mellitus, and Hyperlipidemia
Hypertension, Obesity, Type II Diabetes Mellitus, and Hyperlipidemia
INTRODUCTION
Assessment of a patient’s risk for cardiovascular disease had traditionally required an evaluation of the following factors:
Is there a family history of myocardial infarction (MI) or cerebrovascular accident (CVA) in relatives at an age of <55 years?
Does the patient smoke and if so, how many cigarettes per day?
Is the patient hypertensive?
Does the patient have an abnormal lipid profile?
Is the patient obese?
Does the patient have diabetes mellitus? (In adults this is more often type II.)
Does the patient exercise on a regular basis?
These assessments have been the purview of the internist or family practitioners who care for patients who are older and have exhibited a number of these risks. Unfortunately, these factors are now present in the pediatric population with an increasing frequency so that the pediatrician now needs to evaluate and address them. This changing paradigm forms the basis of this chapter.
EPIDEMIOLOGY
Hypertension has become an increasingly common problem over the past 20 years and the incidence has been rising at an alarming rate. Fixler et al. studied children in the Dallas school system in the 1970s and found that 8% of them had a blood pressure reading above the 95th percentile for age when a single reading was taken. However, fewer than 2% of children had three such readings when these were obtained at separate visits. In contrast, studies done in 2002 showed that the incidence of hypertension when blood pressures were taken in children on three separate visits had risen to 9.5%.
The incidence of obesity and of type 2 diabetes mellitus has also risen dramatically and parallels the rise in childhood hypertension. The increase in obesity and type 2 diabetes mellitus is most striking in adolescent boys; in particular, Hispanic and African-American adolescents are at highest risk for obesity
(Table 13.1). There is also a direct correlation between the increased incidence of obesity and Type II diabetes mellitus. In the adult population, metabolic syndrome is a recognized entity and includes three of the following five elements:
Obesity
Hypertension
Insulin resistance
Hyperlipidemia
Hyperglycemia
This syndrome is associated with a very high risk of cardiovascular and cerebrovascular disease. The alarming phenomena in pediatrics is that 28% to 30% of boys who are overweight (>95 percentile) will have three or more of the elements of metabolic syndrome. This indicates that they are at a much higher risk of early myocardial infarction or
cerebrovascular accident than were prior generations who did not demonstrate these criteria until middle age.
HYPERTENSION
Definitions
Blood pressure nomograms are similar to growth charts for infants and children
(Table 13.2). Children whose blood pressure falls between the 90th and 95th percentiles have
borderline hypertension, and those whose blood pressure is consistently between the 95th and 99th percentiles have
significant hypertension. Children whose blood pressure is higher than the 99th percentile for age are considered to have
severe hypertension.
The study by Fixler et al. illuminated two points regarding the diagnosis of hypertension in children. First, the blood pressure may be labile, and therefore repeated measurements are required before any evaluation or treatment is considered. Within a single visit, the blood pressure may vary markedly, and efforts should be made to document pressures on at least three visits before an investigation into possible causes is initiated.
A second important consideration, especially in older or larger children, is to make sure that the blood pressure cuff covers at least two thirds of the upper arm. The use of a cuff that is smaller than recommended, a particularly common occurrence in athletic or obese adolescents, will result in a falsely elevated pressure.
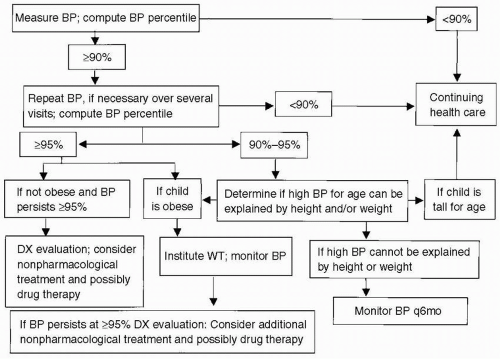
Etiology
Once the cuff size has been determined to be appropriate and the blood pressure is seen to be consistently elevated, the evaluation and treatment outlined in the algorithm shown in
Figure 13.1 can be applied.
Patients whose blood pressure is above the 99th percentile for age are candidates for a more thorough evaluation. The higher the pressure, the more urgent it is to evaluate, and the more likely it is that a cause of the hypertension will be identified.
The causes of hypertension by age are listed in
Table 13.3. Note that renal disease and coarctation of the aorta are prominent in the
younger age groups.
Historical points that help determine the cause of hypertension include a detailed family history and evidence of renal parenchymal disease (e.g., a history of urinary tract infections or abnormal findings on prenatal ultrasonography). Inquiries should also be made to determine whether the patient has episodes of sweating, flushing, and palpitations, which are symptomatic of a pheochromocytoma. Without such symptoms, it is unlikely that a tumor will be found. If they are present, it is essential to obtain 24-hour urine studies for vanillylmandelic acid to detect catecholamine excess.
Two lesions that should be considered during the physical examination are:
Only gold members can continue reading.
Log In or
Register to continue
Related

Full access? Get Clinical Tree


Get Clinical Tree app for offline access