CONTENTS
Anthropometric and Other Measurements
INDICATIONS FOR USE
Intestinal failure (IF) is defined as a condition resulting in an inability to maintain hydration and electrolyte and nutritional status without intravenous support. For many patients with IF, home parenteral nutrition (HPN) is a life-saving modality when IF extends beyond the hospital stay. In the 1970s, HPN became more readily available to patients with infusion pharmacy and homecare services becoming involved in the treatment of these patients. Over the last several decades, HPN providers have reported the main causes of IF, leading to the initiation of HPN [1]. Commonly reported conditions are listed below [1–3]:
• Inflammatory bowel disease (IBD)
• Bowel ischemia
• Short bowel syndrome (SBS)
• Radiation enteritis
• Motility disorder
• Gastrointestinal (GI) fistulae
• Bowel obstruction
Not all patients with IF are appropriate for HPN due to the complexity of the therapy. Determining appropriateness requires a team of nutrition professionals, preferably a nutrition support team (NST), to evaluate nutritional status, GI function, and disease severity of each patient leading to the need for HPN. Specifically, these nutrition professionals include a physician, registered dietitian (RD), registered nurse (RN), pharmacist, social worker, and case manager [4]. This chapter deals primarily with adults requiring HPN. Pediatric HPN is discussed in Chapter 3 with additional references.
The physician oversees the full HPN evaluation process and puts extensive emphasis on conducting a thorough evaluation of the GI tract. Briefly, the RD works with the patient to establish a nutrition prescription to achieve one or several nutrition-related goals. Typical goals include losing, maintaining, or gaining weight and/or to correct or prevent micronutrient deficiencies and dehydration. The RD along with the RN contributes to educating the patient on documenting daily weights, temperatures, and intake and output records. In addition to educating the patient on HPN procedures, the RN assists the patient in selecting a vascular access device (VAD). This is an essential component of the HPN process as the RN ensures that the patient understands the risks and benefits to each VAD prior to making a selection (see Chapter 10). Once the VAD is selected, education on care ensues to allow the patient to be autonomous with the VAD at discharge. The pharmacist inspects the PN solution for stability and compatibility and provides recommendations for medication management in the HPN solution. Cognitive and psychosocial concerns are evaluated by the team social worker with the goal of assessing patient safety with a VAD and intravenous therapies [5,6]. Also, the social worker evaluates the home environment to ascertain if electricity, running water, and telephone access are suitable [7]. Lastly, owing to the extraneous costs of HPN, the case manager will confirm the indication for HPN with the insurance company and verify insurance benefits.
A proficient case manager is critical to preparing the patient for discharge on HPN to ameliorate costs associated with the therapy. Accurately documenting a patient as having permanent IF (>90 days) requiring HPN is critical for financial reimbursement [8]. Knowledge of this documentation is critical for determining insurance benefits (see Chapter 11). Many patients utilize Medicare or Medicaid for HPN coverage, but the majority rely on private insurance to supplement their primary insurance coverage [8]. Determining insurance coverage early on in the discharge process and appropriately documenting the indications for HPN in the medical record is key. Documentation of IF and concurrent insurance approval permits the NST to complete the education sessions and stabilize the PN formula for discharge.
INITIATING HPN
Initiation of HPN can occur in the hospital or home; however, hospital initiation is favored to minimize risk in certain cases. The American Society of Parenteral and Enteral Nutrition (A.S.P.E.N.) recommends hospital initiation for patients with severe medical conditions and/or electrolyte disorders [9]. This chapter will primarily address initiation of PN in the hospital. Initiation of PN in the hospital (or home) should only be started once all significant electrolyte abnormalities are corrected and the patient is metabolically stable. Once electrolyte status is stable, initiating a low-dextrose PN solution on the first day of therapy is warranted to prevent adverse events (i.e., severe hyperglycemia, cardiac dysfunction). In cases of extreme malnutrition or organ dysfunction, reaching the caloric goal may take several days to achieve and daily monitoring of laboratory parameters and weights is necessary to safely advance the PN solution. When the low-dextrose PN is tolerated (i.e., no significant electrolyte or blood sugar abnormalities), the caloric content of the solution can slowly be increased to goal calories. Once a patient is identified as appropriate for HPN, a nutrition-related goal for the PN prescription should be established, as well as other steps in the discharge process (see Figure 9.1). Patients who have an appropriate indication for PN in the home, are clinically stable, have proper access for HPN, and are capable of being educated in the safe administration of HPN, may be initiated in the home setting [9].
PN PRESCRIPTION
Macronutrient, fluid, and micronutrient components of the PN prescription are established based on the nutrition assessment completed by the RD and the nutrition-related goals of each patient. These nutrient components are established prior to initiation and can then be adjusted in response to therapy as needed [7,10]. Total energy needs are established based on the patients’ long-term goal to gain, maintain, or reduce total body weight. Calculating energy needs can be determined by multiple predictive equations or by indirect calorimetry. For most patients, 20–30 kcal/kg of body weight is sufficient for weight maintenance [4,10–12]. Yet, patients requiring weight gain may require up to 42 kcal/kg [13]. Of these calories, lipid should be provided to patients unable to consume adequate dietary fat to prevent essential fatty acid deficiency (EFAD). Prevention of EFAD requires a minimum of 3%–4% total calories delivered from an intravenous fat emulsion (IVFE) unless dietary fat absorption is adequate as EFAD can develop within 1–2 weeks on lipid-free PN prescriptions [10,14,15]. Although A.S.P.E.N. recommends that the lipid content not exceed 2.5 g/kg/day, most clinicians utilize a maximum of 1.0 g/kg/day for long-term HPN therapy [10,16–18]. The current US IVFE is soybean oil based; however, newer alternative lipid sources may allow for a more diverse lipid type and therefore administration tolerance [16]. Protein (i.e., amino acids) and carbohydrate (i.e., dextrose monohydrate) requirements fluctuate based on patient tolerance, medical condition, and the response to therapy and therefore, must be adjusted accordingly [10]. Typically, protein should provide 1.2–2.0 g/kg/day depending on body mass and disease severity and delivered as a concentrated amino acid solution ranging from 3% to 20% [10,12]. Carbohydrate needs are met by infusion of a dextrose monohydrate solution ranging from 5% to 70% with each gram supplying approximately 3.4 kcal. Fluid needs can be estimated by providing 30–40 mL/kg of dry weight [10]. Ultimately, fluid delivery should cover GI and insensible losses while allowing for a minimum of 1000 mL of urine daily for the adult patient [2,4,19]. Electrolyte, vitamin, and mineral additives should be added to the PN bag daily and adjusted based on individual needs. Estimated micronutrient requirements for parenteral nutrition solutions have been reviewed and guidelines are available for dosing [10].
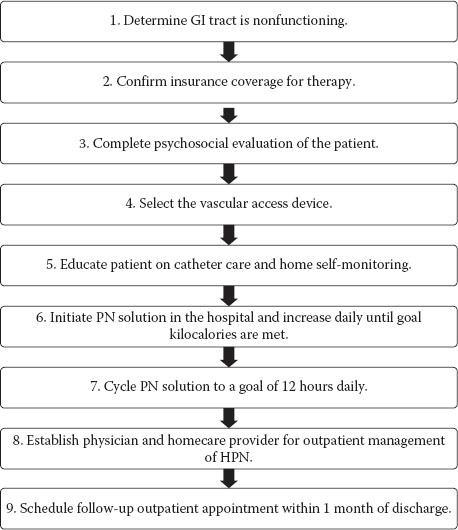
FIGURE 9.1 Steps for discharging a patient on home parenteral nutrition.
With ongoing drug shortages affecting the HPN prescription of many patients with IF, tactics for preventing micronutrient deficiencies have been suggested [20]. Specifically, these guidelines recommend that multivitamin (MVI) and multiple trace element (MTE) solutions should be given orally in those HPN patients with adequate functionality of the GI tract to tolerate and absorb oral doses. In patients without adequate functionality of the GI tract, intravenous MVI and MTE solutions should be reduced from daily to 3× per week [20].
Once the nutritional goals are established, the clinician formulates the PN solution as a 3-in-1 (carbohydrate, lipid, and protein delivered in the same bag) or 2-in-1 (carbohydrate and protein delivered in the same bag and lipids given separately). Several factors determine how the PN solution is formulated, such as fluid requirements, stability parameters, presence of organ failure (i.e., hepatic, renal, and/or pulmonary diseases), and energy needs [10,21]. It is not uncommon for a patient to receive 2-in-1 solutions 6/days per week and a 3-in-1 solution for the remaining day to meet lipid and/or caloric requirements. Guidelines for maintaining stability and compatibility in 3-in-1 admixtures are listed in Table 9.1.
Stability Guidelines for 3-in-1 Admixtures
Nutrient | Parameters |
Macronutrient | ≥4% Amino acid |
≥10% Dextrose | |
≥2% Lipid | |
Divalent cations | Between 16 and 20 mEq/L |
Iron |







