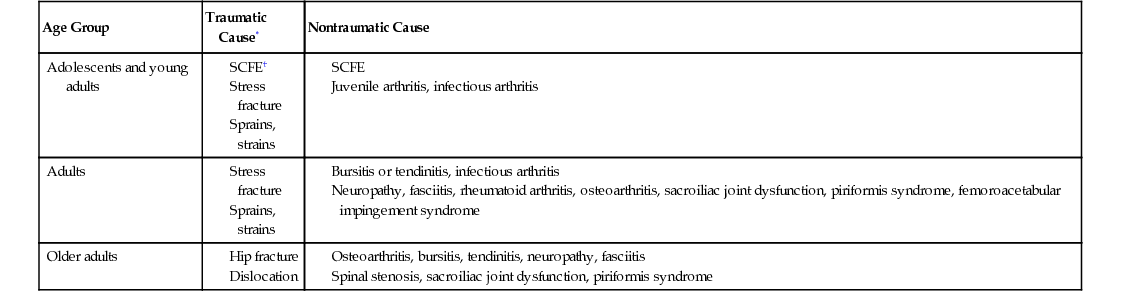
Ann S. Bruner-Welch Hip pain is a common complaint in primary care. It is a major source of discomfort and functional limitation, particularly in older patients, with a long list of potential causes.1–3 It is helpful, therefore, to consider hip anatomy, patient age, and preceding history in teasing out the problem.4 An accurate diagnosis and appropriate management are important in reducing the burden for both the patient and the family. Hip pain may be broadly defined as any sensation of pain immediately surrounding or within the pelvic girdle. Limitations in range of motion are not uncommon, and activity or weight bearing frequently increases symptoms.5 Because hip pain is a symptom and not a specific disease entity, there is no epidemiologic pattern that describes the prevalence and incidence. Major causes of hip pain differ across age groups and may be categorized as traumatic or nontraumatic (Table 178-1). TABLE 178-1 Causes of Hip Pain and Age Groups Commonly Affected A review of hip and pelvic anatomy is the key to understanding the potential source of pain. The hip, like the shoulder, is a diarthrodial ball-and-socket synovial joint. The ball and socket of the hip joint is made up of the head of the proximal femur and the acetabulum or socket of the pelvis.6 The acetabulum is composed of the ischium, pubis, and ilium within the pelvis. A cartilaginous labral lip makes the socket of the acetabulum deeper for stability but maintains flexibility for greater range of hip motion. Strong fibrous, stabilizing ligaments form the capsule that covers the entire hip joint. Articular cartilage covers the bone ends. Completely lining the capsule and extending down to the neck of the femur is the synovial membrane; it secretes synovial fluid, which provides lubrication for motion. Fluid-filled sacs (or bursae), found in spaces among the tendons, ligaments, and bones, reduce friction over bone prominences and permit ease of motion.6 The primary functions of the hip are weight bearing and locomotion. The muscles of the hip are essential in maintaining upright stability and gait. The muscles of the hip may be classified into five functional groups according to their action: abductors, flexors, adductors, extensors, and rotators. Musculotendinous pain of the hip may contribute to distortions of gait, producing a limp. Any one of these structures may become inflamed, stretched, torn, infected, or worn out, causing pain. Crystalline deposits within the joint or surrounding tissues may also cause tissue destruction and pain.7 In growing children, changes, injury, or irritation at growth plates can also cause pain.7,8 The underlying cause of the pain is the result of the actual pathophysiologic process. Active individuals can stress the bone and supporting soft tissue. Muscle, tendon, or ligament strains and sprains are common in more active individuals. Labral tears also typically occur in active individuals. Very active individuals can develop stress fractures.9 Modulation in activity may be necessary for the joint to heal and the pain to resolve. Bursitis (see Chapter 173) is an irritation and inflammation of the bursa, usually over bone prominences such as the greater trochanter. It is common in individuals with lateral hip pain on ambulation and at night.1–3,10 Osteoarthritis (OA) (see Chapter 184) is a breakdown or degeneration of the cartilage within the joint, causing bone ends to rub.1–3,11 Rheumatoid arthritis (RA) (see Chapter 218) is an inflammatory, autoimmune, destructive joint process that frequently affects multiple joints and causes synovitis, pain, and stiffness.1–3,12 The joint involvement in RA is often symmetric; therefore both hips may be painful. Psoriatic arthritis (see Chapter 215) is more common in men than in women and should be considered in individuals diagnosed with psoriasis.5 Gout and pseudogout (see Chapter 176) leave crystalline deposits within the joint, leading to joint inflammation, acute-onset pain, and eventual cartilage destruction.7 Avascular necrosis is loss of blood supply and subsequent death of subchondral bone tissue; it is often related to trauma, alcohol intoxication, sickle cell anemia, or corticosteroid use.1–3,13 Protease inhibitors, RA, or systemic lupus erythematosus (see Chapter 219) can also be causative. Avascular necrosis can occur in a number of sites in the body, including the femoral head, and can be bilateral. The cartilage remains intact; however, the bone beneath it becomes flattened and misshapen.13 Fractures and hip dislocations in younger to middle-aged people are most commonly associated with significant trauma, such as motor vehicle accidents or significant falls. They may be followed in primary care once they are stabilized. Low-impact trauma should not produce a significant fracture in young healthy adults. Fragility fractures at any age should prompt further bone density testing and endocrinology evaluation, including looking for secondary causes of osteopenia or osteoporosis (see Chapter 182), such as vitamin D deficiency, hyperparathyroidism, anorexia nervosa, female athlete triad, or other reversible causes of brittle bones.1–3,14 Hip dislocations should be considered if there is a history of hip replacement surgery or congenital hip dislocation. Infection (see Chapter 179) is uncommon but can be a devastating cause of rapid-onset hip pain and fever.1–3,15 It can become indolent and recurrent, particularly with more virulent microbes. Recent dental work, skin infection, endocarditis, and intestinal procedures are frequent sources, particularly if a prosthesis is in place. In the adolescent and young adult, Neisseria gonorrhoeae is the most common causative organism.15 In adults of all ages, Staphylococcus aureus is the usual source of infection, although other pathogens may be implicated. Methicillin-resistant Staphylococcus aureus (MRSA) is becoming a more common pathogen.15 Neoplasms can originate in the bone or metastasize to it and can cause anything from odd bone growths along the cortex to benign or destructive cystic lesions to complete bone destruction. All patients with questionable x-ray findings should be referred to a specialist promptly for further evaluation.1–3,16 Multiple myeloma and osteosarcoma are the most common primary metastatic tumors (see Chapter 172).16 These tumors frequently manifest as pathologic fractures. Benign bone tumors are frequently found incidentally on x-ray examination.14 Hip pain can also be referred from the back or sacroiliac joint. This cause can frequently be teased out during evaluation because hip motion does not affect the discomfort, but back or sacroiliac mobilization does.1–6 Inguinal hernias can also cause hip pain and can be discovered during examination.1–6 This anterior hip or groin pain or bulging usually increases with bearing down or lifting of heavy objects and is frequently associated with a history of straining before onset of pain. Femoroacetabular impingement (FAI) syndrome is becoming recognized as a frequent cause of hip pain. Bone spurs develop along the edges of the acetabulum or femoral head, causing it to deform and become irregularly shaped, or the socket becomes deeper than it should be, or angled more posteriorly than normal. Any of these changes from normal increases friction between the socket and the femoral head or neck, and the shape mismatch increases cartilaginous wear and tearing of the labrum seal around the joint.1–3,17,18 There are three types of impingement, depending on whether there is a cam action or pinching of the rim of the acetabulum, irritation of the femoral head or neck, or both. When symptoms develop, it usually indicates that damage to either the labrum or cartilage has occurred.17,18 Hip pain is much less common in children than in adults.7,8 Congenital hip dislocation should be considered in infants and subsequent hip dysplasia in young children.1–3,7,8 Apophysitis is a tendinitis in the growing skeleton found in childhood through young adolescence.7,8 Legg-Calvé-Perthes disease is avascular necrosis of the femoral head found mostly in 4- to 8-year-old boys.7,8 Transient synovitis, a benign, self-limiting, but painful condition, is the most common cause of pain during childhood.7,8 It can occur in growing bones, and the incidence typically decreases by age 12. Age 2 to 5 is most commonly affected age group. Causes can include allergic, traumatic, viral, or poststreptococcal toxic synovitis. Fever is rare. Restricted hip abduction is the most sensitive range of motion limitation.6 Pain is worse in the morning and eases with activity.7,8 Ruling out juvenile arthritis and sepsis is especially important, and following closely for the possible development of Legg-Calvé-Perthes disease is clearly indicated. Slipped capital femoral epiphysis (SCFE), in which the growing femoral head and growth plate slip in relation to the remainder of the head and femoral neck, is most common in 11- to 14-year-olds and in boys more than girls. It can be traumatic or atraumatic. It is more common during periods of rapid growth, is associated with obesity, and can be bilateral.1–3,7,8
Hip Pain
Definition and Epidemiology
Age Group
Traumatic Cause*
Nontraumatic Cause
Adolescents and young adults
Adults
Older adults
 Orthopedic consultation is indicated for patients with suspected hip dislocation, fracture, sepsis, end-stage degenerative joint disease that is failing to respond to conservative treatment, or osseous abnormalities that are seen radiographically.
Orthopedic consultation is indicated for patients with suspected hip dislocation, fracture, sepsis, end-stage degenerative joint disease that is failing to respond to conservative treatment, or osseous abnormalities that are seen radiographically.
Pathophysiology





Full access? Get Clinical Tree


