52 High-Frequency Ventilation
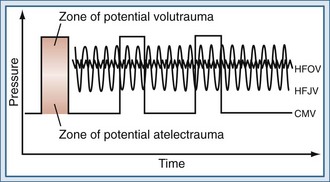
Over the last 30 years, our understanding of the potential harm of mechanical ventilation has evolved, and it has been clearly demonstrated that lung injury may occur through injurious mechanical forces generated during mechanical ventilation. Potential causes of lung injury include gross air leaks (barotrauma), diffuse alveolar injury due to overdistension (volutrauma), injury due to repeated cycles of recruitment and derecruitment (atelectrauma), and injury due to the release of mediators from the lung (biotrauma).1,2 Importantly, volutrauma and atelectrauma lead to biotrauma, which affects not only the lung but may also contribute to multiple organ dysfunction, the major cause of death in patients with ARDS. Lung-protective mechanical ventilation strategies aim to reduce these injurious forces and subsequent lung damage while providing adequate ventilation and oxygenation. The mechanics of high-frequency ventilation, particularly high-frequency oscillatory ventilation (HFOV), make it particularly well suited to protect the lung, and there is growing clinical experience with the use of high-frequency ventilation as an alternative to conventional mechanical ventilation or as salvage therapy in patients failing conventional ventilation strategies.
 Description and Classification
Description and Classification
High-Frequency Positive-Pressure Ventilation
HFPPV was first described in 1969 as an experimental technique3 and has subsequently found only limited clinical use in specialized upper-airway surgical procedures and bronchoscopy.4 Published clinical experience with HFPPV is largely limited to neonatal populations. One meta-analysis in newborn infants found that synchronized mechanical ventilation delivered as HFPPV was associated with reduced barotrauma and shorter hospital stay compared with conventional mechanical ventilation (CMV),5 but the effect on mortality and chronic oxygen dependency was unclear. In adult patients, HFPPV has been used only in specialized applications in the field of anaesthesia.6–8
High-Frequency Percussive Ventilation
High-frequency percussive ventilation (HFPV) is a hybrid mode that combines the principles of high frequency and CMV using a proprietary mechanical ventilator.9 A conventional ventilation circuit is fitted with a gas-driven piston at the end of the endotracheal tube. The reciprocating piston generates pressure oscillations at 3 to 15 Hz, with short expiratory times that are superimposed on the conventional inspiratory-expiratory pressure waves. The high-frequency beats are delivered in bursts to generate auto-PEEP through breath stacking, and then are interrupted to allow alveolar pressure to return to baseline. It has been hypothesized that the auto-PEEP generated improves alveolar recruitment without exposing the alveoli to the high peak airway pressures that would be generated with comparable CMV. Although the high-frequency pressure oscillations are driven actively in both directions, the bulk of exhalation is passive, from the underlying CMV breaths. The high-frequency percussion also provides some internal mucokinesis, potentially improving pulmonary toilet and reducing endotracheal suctioning requirements.10 Indeed, it may be because of this property that HFPV has been most commonly used in adult patients with inhalational injury, burns, and trauma.
High-Frequency Jet Ventilation
High-frequency jet ventilation (HFJV) employs a small-aperture nozzle inserted into the endotracheal tube in order to direct a high-pressure stream of gas into the lung (Figure 52-1). During inspiration, a high-pressure jet streams into the proximal airways, entraining air from the circuit, and tidal volume is therefore largely dependent on the Venturi and Coanda effects. The parameters controlled by the clinician are frequency, inspiratory time, jet drive pressure, and PEEP applied through the ventilator circuit. Tidal volumes are determined by the jet driving pressure and inspiratory time (i.e., larger tidal volumes can be delivered by increasing jet drive pressure and inspiratory time). Tidal volumes will also be augmented by using a larger jet catheter and a larger endotracheal tube, which increase the amount of jet flow and gas entrainment, respectively. Because expiration is passive, gas trapping may occur at higher frequencies with progressively shorter expiratory times.
A complication specific to HFJV is traumatic upper airway injury. The high-velocity inspiratory jet may cause direct trauma to the proximal airways, and necrotizing tracheobronchitis is a recognized complication of HFJV in both infants and adults.11,12 Gas conditioning during HFJV, particularly humidification and warming, is also problematic. Although the gas entrained from the proximal circuit is warmed and humidified, the gas injected from the jet nozzle expands and cools, compromising the overall conditioning of the inspired gas. It has also been hypothesized that high gas flow rates and rapid increases in lung volume could cause lung injury through the generation of shear forces at the interface of adjacent compliant and atelectatic lung units.13
The clinical utility of HFJV is specific to certain clinical settings such as pulmonary air leak syndromes, when the ability to achieve adequate gas exchange with lower peak airway pressures may be advantageous.14 In addition, the decreased reliance on bulk flow with HFJV may improve gas distribution and gas exchange in the presence of large air leaks, although this theoretical advantage has not been borne out in clinical studies.15
The published clinical experience with HFJV in acute respiratory failure remains small, and to date, the greatest clinical experience is in the neonatal and pediatric populations and in anesthesia for airway stability during respiratory tract surgery. There is limited research in its utility in adult respiratory failure, although many intensive care units (ICUs) have sizable anecdotal experience. Comparative clinical trials have shown that high-frequency jet ventilation is safe and offers improved oxygenation and ventilation compared with CMV, while improving respiratory parameters and decreasing required peak pressures.16–18 None of these trials, however, demonstrated a significant survival advantage.
High-Frequency Oscillatory Ventilation
During HFOV, a piston pump oscillates a diaphragm at frequencies between 3 and 15 Hz (180-900 breaths/min) to create pressure waves in the ventilator circuit (see Figure 52-1). Because the diaphragm is actively driven in both directions, the ventilator creates both inspiratory and expiratory pressure waves, meaning that expiration is also active. The use of active expiration distinguishes HFOV from other forms of high-frequency ventilation, in which expiration is passive and dependent on the elastic recoil of the respiratory system. Active expiration may be advantageous in controlling CO2 and preventing hyperinflation. Indeed, HFOV has been shown to be associated with less gas trapping than other forms of high-frequency ventilation.19 The mean airway pressure is maintained by a resistance valve in the circuit, together with the inspiratory bias flow. Changes in alveolar pressure are kept low by small excursions of the piston. Humidification is achieved by passing the bias flow of gas through a humidifier.20
 Mechanisms of Gas Transport with High-Frequency Oscillatory Ventilation
Mechanisms of Gas Transport with High-Frequency Oscillatory Ventilation
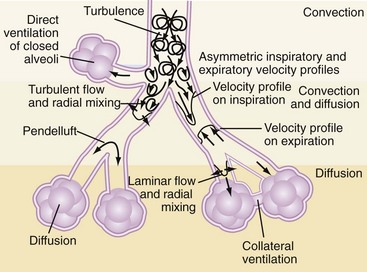
During CMV, gas exchange is largely related to bulk flow of gas to the alveoli. However, since the tidal volumes generated during HFOV may be smaller than the anatomic dead space, ventilation relies on alternative gas exchange mechanisms related largely to enhanced gas mixing within the lung. These gas exchange mechanisms are summarized in Table 52-121 and Figure 52-2. Experimental models suggest that in contrast to CMV, CO2 elimination is a product of the frequency and the square of the tidal volume (VCO2 α = f × VT2)22 such that adequate CO2 elimination may become problematic as tidal volumes decrease, unless accompanied by proportionately larger increases in frequency. Regardless, clinical experience has demonstrated that adequate gas exchange can be achieved in adults with HFOV using frequencies in the 8- to 10-Hz range, delivering tidal volumes that are less than anatomic dead space.23
TABLE 52-1 Mechanisms of Gas Exchange During High-Frequency Oscillatory Ventilation
| Site | Proposed Mechanism |
|---|---|
| Proximal airway | Bulk flow—remains an important mechanism of gas transport in proximal airways |
| Mid-airway | Pendelluft—phenomenon of regional gas movement that occurs as a result of heterogeneity in alveolar filling and emptying rates. Adjacent lung units with different time constants may fill at different rates during inspiration. Following inspiration, there is redistribution of inspired gas from full, fast-filling units to slower-filling units, augmenting gas exchange.9 Taylor dispersion—enhanced diffusion augmented by radial transport mechanisms Asymmetrical velocity profiles—results in a net convective transport of material, especially at airway bifurcations. Fresh gas streams toward alveoli along inner airway walls, while “alveolar” gas streams cranially along outer airway wall. |
| Distal airway | Cardiogenic mixing—rhythmic contraction of heart promotes peripheral gas mixing by generating flow within neighboring parenchymal regions Collateral ventilation—gas exchange between noncommunicating neighboring alveoli via collateral channels |
From Chang HK. Mechanisms of gas transport during ventilation by high-frequency oscillation. J Appl Physiol. 1984;56(3):553-563.
 Rationale for High-Frequency Oscillatory Ventilation
Rationale for High-Frequency Oscillatory Ventilation
In the last few decades, there has been an enormous increase in understanding of the effects of mechanical ventilation on the lung and elucidation of VILI and its pathophysiology, namely volutrauma, atelectrauma, and biotrauma. Furthermore, the clinical relevance of VILI was solidified by a landmark study published by the ARDS Network in 2000 that demonstrated a 9% absolute mortality reduction in patients with ARDS ventilated with tidal volumes of 6 mL/kg ideal body weight compared with 12 mL/kg.24
HFOV would appear to be the ideal lung-protective ventilation strategy in patients with ALI/ARDS because of two principal properties: (1) prevention of VILI by delivery of small tidal volumes with limitation of alveolar overdistention and (2) promotion of alveolar recruitment through application of a higher mean airway pressure than can be safely applied with CMV, promoting more alveolar recruitment and avoiding cyclic opening and closing of alveolar units throughout the respiratory cycle. Indeed, there is a wealth of preclinical animal data demonstrating that compared with both injurious and lung-protective conventional ventilation, HFOV is advantageous in terms of gas exchange, markers of inflammation, and lung pathology scores.25
Does High-Frequency Oscillatory Ventilation Truly Deliver Small Tidal Volumes?
Although tidal volumes are not measured directly on the oscillator that is commercially available in the United States, several investigators have measured delivered tidal volumes. In a sheep saline-lavage model of ALI, Sedeek et al. measured delivered tidal volumes with a pneumotachograph26 and found that HFOV applied with a frequency of 4 Hz and pressure amplitude of 60 cm H2O resulted in tidal volumes of 4 mL/kg—not large, but not as small as had been anticipated. More recently, however, Hager and colleagues measured tidal volumes in adults with ARDS receiving HFO using a hot-wire anemometer, which may provide more accurate measurements. These investigators found that usual tidal volumes delivered during adult HFOV were indeed small, in the 1 to 2 mL/kg range, and that frequency27 rather than pressure amplitude was the dominant determinant of tidal volume in adults with ARDS. These authors emphasized that while low tidal volumes can be delivered during HFO, at low frequencies, tidal volumes may be larger than anticipated. This suggests that a strategy that achieves acceptable CO2 clearance while employing the highest tolerated frequency is likely to be most lung protective. To practically achieve these goals, we generally use a relatively high power set to achieve a pressure amplitude (delta P [ΔP]) of 90 cm H2O, and then adjust frequency as high as tolerated to achieve an adequate pH (>7.25), at times using a partial leak around the endotracheal tube cuff to facilitate CO2 clearance and higher frequency tolerance.



Full access? Get Clinical Tree


