Fig. 53.1
Nevro Corp. Senza IPG and SCS leads capable of HF10 therapy
Clinical Studies Demonstrating Efficacy of High-Frequency Stimulation
There is increasing clinical evidence on the efficacy of high-frequency stimulation, which began with the feasibility study by Tiede and colleagues, published in 2013 [2]. The study was performed in 2007–2008, utilizing temporary SCS leads in 24 patients with the diagnoses of low back pain and Failed Back Surgery Syndrome (FBSS). The subjects first received conventional stimulation for 4–7 days, then high-frequency stimulation for an additional 4 days via the same percutaneous leads [2]. VAS pain scores were shown to be further improved with high-frequency stimulation, and more patients preferred the high-frequency SCS mode in this study [2].
In 2013, a prospective, open-label, multicenter European clinical trial with 10 kHZ SCS was published [3]. Seventy-two patients with lower back and/or leg pain , along with the diagnosis of Failed Back Surgical Syndrome, were implanted with commercially available HF10 SCS therapy. Most of the subjects suffered from axial low back pain without radiculopathy, which is generally considered more challenging to treat with SCS [3, 4]. Over a 6-month follow-up, study subjects demonstrated significant improvements in VAS pain scores, Oswestry Disability Index scores, and sleep patterns [3]. Similar SCS benefits were also demonstrated at 24 months post-implantation, suggesting that HF10 therapy is likely to produce sustained pain relief without tolerance on a long-term basis [4].
The pivotal study demonstrating the efficacy and superiority of HF10 therapy to traditional SCS was the SENZA-RCT study, published in 2015 [1]. The SENZA-RCT randomized 198 patients with back and/or leg pain to either traditional, low-frequency SCS (Boston Scientific™ Precision Plus), or HF10 SCS therapy, with Nevro SENZA® system [1]. The responder rates to treatment were significantly higher in the HF10 therapy arm for the 12-month duration of the study [1]. The 24-month data also reflected similar results, underscoring the efficacy and durability of HF10 therapy [5]. VAS scores were reported to be much lower for both back and leg pain in the HF10 therapy arm subjects in the SENZA-RCT study [4, 5]. Moreover, HF10 therapy subjects reported improved functional capacity at a statistically significant level, which was superior to the traditional, low-frequency arm subjects. Although both arms demonstrated a reduction in opioid use, the HF10 therapy subjects reduced their opioid usage at a higher rate. Subject satisfaction, reported by the patients, was also significantly higher throughout the entire study [4, 5]. Adverse events were rare in both arms, underscoring the safety of SCS, regardless of device choice throughout the study [4, 5].
Although the evidence for low back and leg pain control has established HF10 therapy as a superior choice for this condition, additional studies are warranted and underway to evaluate the efficacy of HF10 therapy in various other indications.
Trial Procedure for HF10 Therapy
Positioning
The patient is placed in the prone position, in the usual manner for all dorsal column SCS placements. A pillow or two is placed underneath the patient’s abdomen to minimize lumbar lordosis. Access to the epidural space is most likely from the upper lumbar area of the spine, using a paramedian approach. The authors prefer L1 and L2, in order of preference, for epidural access.
Anesthesia
For SCS trials, patients may be sedated using IV sedation or other anesthesia, which is based on the surgeon’s preference. The patient need not be awake, as paresthesia mapping is not necessary with HF10 therapy. Local anesthetic of choice should be used over the intended trajectory of a 14-gauge Tuohy needle in the deeper fascia, in order to minimize soft tissue discomfort. Although paresthesia mapping in the operating room is unnecessary with HF10 therapy, communication with the patient is critical, in order to allow early detection of adverse incidental events, such as inadvertent spinal cord, or nerve injury during the procedure. Therefore, the authors would recommend refraining from deep anesthesia in the trial patient population.
Lead Placement
Using fluoroscopic guidance , the lumbar interlaminar space is visualized, with the spinous processes positioned at midline. The upper endplate of the target interlaminar level is aligned by tilting the image intensifier on the fluoroscope toward the feet of the patient. This will ensure optimal trajectory and direction toward the epidural space for the surgeon. The entry point for the manufacturer-supplied 14-gauge Tuohy needle is approximately medial to the pedicle, at the level below the target interlaminar space. The Tuohy needle is then advanced in a paramedian fashion toward the target laminae (Fig. 53.2).

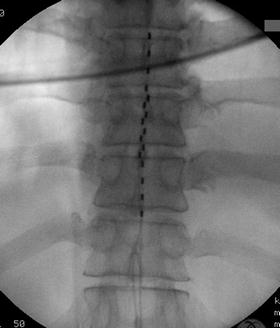
Fig. 53.2
Paramedian approach is used for HF10 therapy similar to traditional SCS needle placement. Needle tip position should be at midline at epidural entry
The Tuohy needle is advanced slowly into the epidural space using a standard loss of resistance technique. The surgeon may prefer to use AP or lateral fluoroscopy for the approach to the epidural space. Nonetheless, the target epidural entry point should be at, or near, the midline, as close as possible to the inferior portion of the spinous process. This approach will allow the most expeditious needle placement, in order to allow the path of least resistance to the epidural midline with the lead (Fig. 53.3). The upper contact of the first lead is placed at the top of the T8 endplate at the anatomical midline. The second lead is subsequently placed in a similar fashion at the anatomical midline, with the uppermost contact at the mid-body of T9 on AP fluoroscopy. Care must be taken to stagger the leads to avoid contact between the leads (Figs. 53.4 and 53.5).

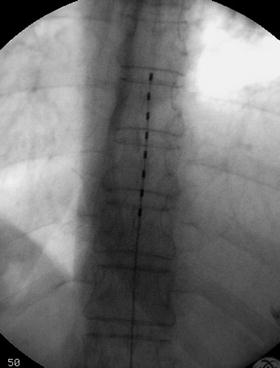
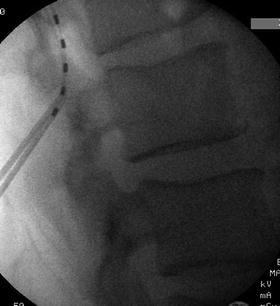
Fig. 53.3
Lateral view of the Nevro SCS lead initial tread into the posterior epidural space
Fig. 53.4
AP view of properly positioned first lead for HF10 therapy with the upper contact at the upper endplate of T8 at the anatomical midline
Fig. 53.5
Lateral view of the second lead placement
The aforementioned studies have demonstrated the best results in low back and leg pain control with this type of anatomical midline placement. The manufacturer, as well as this chapter’s authors, strongly recommend anatomical midline placement of the leads for best results. This is based on the compelling evidence in a number of different peer-reviewed published studies, as well as real world experience. This recommendation is independent of the laterality of the pain pattern in any patient. This approach is most likely to provide the best and most consistent results in all patients with low back and leg pain, who would be candidates for SCS therapy (Fig. 53.6). The leads are then connected to the programmer for an impedance check. This is typically completed within 5–10 s by the representative of the manufacturer. Once the impedance is confirmed, the Tuohy needles and lead stylets are cautiously removed, under live fluoroscopy in the AP view, to ensure prevention of lead migration.
 Pain in the Stroke Rehabilitation Patient
Pain in the Neuromuscular Disease Rehabilitation Patient
Basic Psychopharmacology for the Treatment of Pain in the Rehabilitation Patient
Intrathecal Therapy for the Treatment of Pain in the Rehabilitation Patient
Pain in the Stroke Rehabilitation Patient
Pain in the Neuromuscular Disease Rehabilitation Patient
Basic Psychopharmacology for the Treatment of Pain in the Rehabilitation Patient
Intrathecal Therapy for the Treatment of Pain in the Rehabilitation Patient
 Intra-articular Joint and Bursa Injections for the Treatment of Pain in the Rehabilitation Patient
Intra-articular Joint and Bursa Injections for the Treatment of Pain in the Rehabilitation Patient
 Chiropractic Medicine for the Treatment of Pain in the Rehabilitation Patient
Chiropractic Medicine for the Treatment of Pain in the Rehabilitation Patient



Related posts:
Pain in the Stroke Rehabilitation Patient
Pain in the Neuromuscular Disease Rehabilitation Patient
Basic Psychopharmacology for the Treatment of Pain in the Rehabilitation Patient
Intrathecal Therapy for the Treatment of Pain in the Rehabilitation Patient
Intra-articular Joint and Bursa Injections for the Treatment of Pain in the Rehabilitation Patient
Chiropractic Medicine for the Treatment of Pain in the Rehabilitation Patient
Full access? Get Clinical Tree
