CHAPTER 170
Herpes Zoster
(Shingles)
Presentation
There may be prodromal symptoms that include malaise, nausea and vomiting, headache, and photophobia. Less commonly, there may be fever. During this prodromal stage, which can last several days, there may be accompanying preherpetic neuralgia.
Patients complain of symptoms that range from an itch or tingling to severe lancinating pain, tenderness, dysesthesias, paresthesia, or hypersensitivity that covers a specific dermatome. This discomfort may be precipitated by minor skin stimulation from the patient’s clothes and is characteristic of this type of neurologic pain. After 1 to 5 days, the patient may develop a characteristic unilateral rash. The discomfort may be difficult for the patient to describe, often alternating between an itch, a burning, and even a deep aching pain. Prior to the onset of the rash, zoster can be confused with pleuritic or cardiac pain, cholecystitis, or ureteral colic. The pain may precede the eruption by as much as a few weeks, and occasionally, pain alone is the only manifestation (zoster sine herpete). Although almost exclusively a unilateral disease, in one study, approximately 1% of patients had bilateral involvement.
The early rash consists of an eruption of erythematous macules and papules that usually appear posteriorly first and then spread anteriorly along the course of an involved nerve segment. In most instances, clusters of clear vesicles on an erythematous base will appear within the next 24 hours (Figures 170-1 to 170-3). These continue to form for 3 to 5 days and then evolve through states of pustulation, ulceration, and crusting.
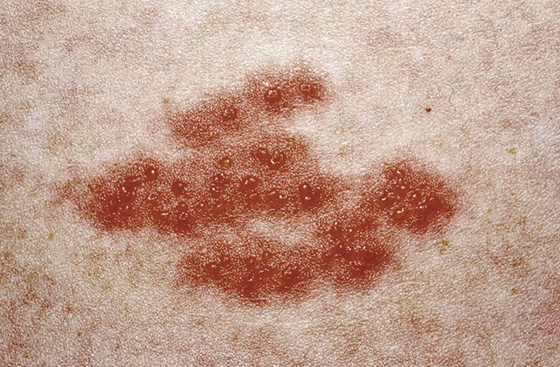
Figure 170-1 Herpes zoster. Classic appearance of grouped vesicles. (From White G, Cox N: Diseases of the skin, ed 2. St Louis, 2006, Mosby.)

Figure 170-2 The vesicles of herpes zoster may at times be hemorrhagic. (From White G, Cox N: Diseases of the skin, ed 2. St Louis, 2006, Mosby.)

Figure 170-3 Herpes zoster infection, typically involving a single unilateral dermatome. (From White G, Cox N: Diseases of the skin, ed 2. St Louis, 2006, Mosby.)
The skin eruption usually is limited to a single dermatome; the most commonly involved dermatomes are the thoracolumbar region and the face. Lesions may involve more than one dermatome and occasionally may cross the midline. With seventh cranial nerve involvement (causing weakness of all facial muscles on one side), the rash will be found in the ipsilateral external ear (called zoster oticus), or vesicles may be seen on the hard palate.
What To Do:
 If it has been 3 days or less since the onset of the rash, prescribe valacyclovir (Valtrex), 1000 mg tid × 7 days; famciclovir (Famvir), 500 mg tid × 7 days; or the much less expensive but more inconvenient acyclovir (Zovirax), 800 mg five times per day × 7 days. If a patient presents later than 72 hours after onset, antivirals may still be considered if new lesions are being formed.
If it has been 3 days or less since the onset of the rash, prescribe valacyclovir (Valtrex), 1000 mg tid × 7 days; famciclovir (Famvir), 500 mg tid × 7 days; or the much less expensive but more inconvenient acyclovir (Zovirax), 800 mg five times per day × 7 days. If a patient presents later than 72 hours after onset, antivirals may still be considered if new lesions are being formed.
 Prescribe analgesics appropriate for the level of pain the patient is experiencing. NSAIDs may help, but narcotics are often required (e.g., oxycodone [Oxycontin, Roxicodone] q6-12h or Percocet q4h). When prescribing narcotics for the elderly, remember to warn them that they are likely to suffer constipation as a side effect (see Chapter 67). Other side effects of opioids include nausea, decreased appetite, and sedation. If the pain is severe, consider referring the patient for an epidural nerve block, which has been successful in relieving the acute pain and may decrease the incidence of postherpetic neuralgia.
Prescribe analgesics appropriate for the level of pain the patient is experiencing. NSAIDs may help, but narcotics are often required (e.g., oxycodone [Oxycontin, Roxicodone] q6-12h or Percocet q4h). When prescribing narcotics for the elderly, remember to warn them that they are likely to suffer constipation as a side effect (see Chapter 67). Other side effects of opioids include nausea, decreased appetite, and sedation. If the pain is severe, consider referring the patient for an epidural nerve block, which has been successful in relieving the acute pain and may decrease the incidence of postherpetic neuralgia.
 There is evidence that treating older patients (60 years of age and older) with amitriptyline (Elavil), 25 mg qd × 90 days, will reduce the risk for postherpetic neuralgia. (There was a 50% decrease in pain prevalence at 6 months compared with placebo.) Coordinate such treatment with a follow-up physician.
There is evidence that treating older patients (60 years of age and older) with amitriptyline (Elavil), 25 mg qd × 90 days, will reduce the risk for postherpetic neuralgia. (There was a 50% decrease in pain prevalence at 6 months compared with placebo.) Coordinate such treatment with a follow-up physician.
 Cool compresses with Burow solution will be comforting (e.g., Domeboro powder, 2 packets in 1 pint of water).
Cool compresses with Burow solution will be comforting (e.g., Domeboro powder, 2 packets in 1 pint of water).
 Dressing the lesions with gauze and splinting them with an elastic wrap may also help bring relief. Superficial infection may be prevented by the use of a topical antibiotic ointment, such as mupirocin (Bactroban) 2% ointment (1 tube, 22 g), applied bid.
Dressing the lesions with gauze and splinting them with an elastic wrap may also help bring relief. Superficial infection may be prevented by the use of a topical antibiotic ointment, such as mupirocin (Bactroban) 2% ointment (1 tube, 22 g), applied bid.
 Secondary infection should be treated with systemic antibiotics, such as cephalexin, 500 mg qid × 7 to 10 days, or azithromycin, 500 mg, then 250 mg qd × 4 days. Always keep in mind the possibility of an infection with community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) (see Chapter 172).
Secondary infection should be treated with systemic antibiotics, such as cephalexin, 500 mg qid × 7 to 10 days, or azithromycin, 500 mg, then 250 mg qd × 4 days. Always keep in mind the possibility of an infection with community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) (see Chapter 172).
 Ocular lesions should be evaluated by an ophthalmologist and treated with topical ophthalmic corticosteroids. Although topical steroids are contraindicated in herpes simplex keratitis, because they allow deeper corneal injury, this does not appear to be a problem with herpes zoster ophthalmicus (Figure 170-4). If the rash extends to the tip of the nose (the Hutchinson sign), the eye will probably be involved, because it is served by the same nasociliary branch of the trigeminal nerve. Look for punctate keratopathy on slit-lamp examination with fluorescein staining, although patients may have only pain, lacrimation, conjunctivitis, or scleritis. Herpes zoster ophthalmicus can result in corneal scarring, uveitis, glaucoma, corneal perforation, or blindness. Patients with AIDS are at risk for developing acute retinal necrosis.
Ocular lesions should be evaluated by an ophthalmologist and treated with topical ophthalmic corticosteroids. Although topical steroids are contraindicated in herpes simplex keratitis, because they allow deeper corneal injury, this does not appear to be a problem with herpes zoster ophthalmicus (Figure 170-4). If the rash extends to the tip of the nose (the Hutchinson sign), the eye will probably be involved, because it is served by the same nasociliary branch of the trigeminal nerve. Look for punctate keratopathy on slit-lamp examination with fluorescein staining, although patients may have only pain, lacrimation, conjunctivitis, or scleritis. Herpes zoster ophthalmicus can result in corneal scarring, uveitis, glaucoma, corneal perforation, or blindness. Patients with AIDS are at risk for developing acute retinal necrosis.
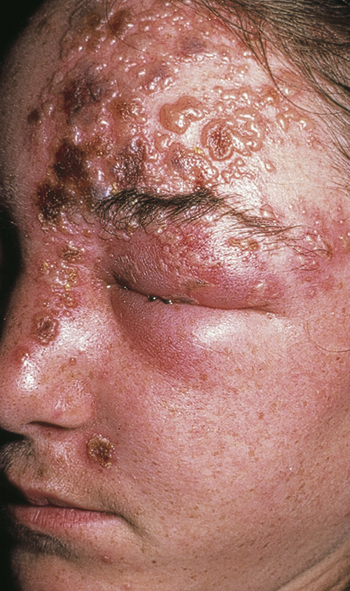
Figure 170-4 Ophthalmologic zoster vesicles and crusting of the top and side of the nose in herpes zoster implies involvement of the nasociliary branch of the trigeminal nerve and eye involvement. (From White G, Cox N: Diseases of the skin, ed 2. St Louis, 2006, Mosby.)
 Until all lesions are crusted, instruct patients to stay away from immunocompromised individuals and pregnant women who have not had chickenpox. Explain that they can transmit varicella (chickenpox) to a susceptible individual.
Until all lesions are crusted, instruct patients to stay away from immunocompromised individuals and pregnant women who have not had chickenpox. Explain that they can transmit varicella (chickenpox) to a susceptible individual.
What Not To Do:
 Do not prescribe systemic steroids to prevent postherpetic neuralgia, especially for patients who are at high risk (i.e., with latent tuberculosis, immunocompromise, peptic ulcer, diabetes mellitus, hypertension, or congestive heart failure). Although they are sometimes recommended to reduce acute symptoms, oral corticosteroids given during the acute phase of the illness have not been shown to reduce the incidence or severity of postherpetic neuralgia.
Do not prescribe systemic steroids to prevent postherpetic neuralgia, especially for patients who are at high risk (i.e., with latent tuberculosis, immunocompromise, peptic ulcer, diabetes mellitus, hypertension, or congestive heart failure). Although they are sometimes recommended to reduce acute symptoms, oral corticosteroids given during the acute phase of the illness have not been shown to reduce the incidence or severity of postherpetic neuralgia.
 Do not initiate a comprehensive diagnostic workup to look for an occult malignancy simply on the basis of zoster. The incidence of cancer among patients with zoster is no greater than that of the general population. Patients with cancers, particularly lymphomas, are, however, at increased risk for zoster. Usually the cancer diagnosis is already known when zoster occurs.
Do not initiate a comprehensive diagnostic workup to look for an occult malignancy simply on the basis of zoster. The incidence of cancer among patients with zoster is no greater than that of the general population. Patients with cancers, particularly lymphomas, are, however, at increased risk for zoster. Usually the cancer diagnosis is already known when zoster occurs.
 Do not use topical antiviral agents. They are not effective and are not recommended.
Do not use topical antiviral agents. They are not effective and are not recommended.
Discussion
Herpes zoster can usually be readily diagnosed from its clinical appearance of typical lesions in a dermatomal distribution. One well-known diagnostic caveat is that the pain and rash do not cross the midline; however, it is not impossible for the disease to be bilateral and involve more than one dermatome, and multidermatomal zoster may be the presenting finding for human immunodeficiency virus (HIV).
Bell’s palsy (see Chapter 5) following zoster dermatitis of the external ear canal is well known and can be part of the Ramsay Hunt syndrome (Figure 170-5). The virus invades the facial nerve, especially the geniculate ganglion, and occasionally the auditory nerve, and can produce the peripheral seventh-nerve palsy, along with hearing loss, vertigo, and taste dysfunction.

Figure 170-5 Ramsay Hunt syndrome. (From White G, Cox N: Diseases of the skin, ed 2. St Louis, 2006, Mosby.)
Antiviral therapy has been shown to shorten the duration of viral shedding, halt the formation of new lesions more quickly, accelerate the rate of healing, and reduce the severity of acute pain. Herpes zoster ophthalmicus is a particularly important variant, and these patients should definitely receive antiviral therapy early with the goal of preventing ocular complications.
Antiviral treatment is generally recommended for all patients of any age with severely symptomatic herpes zoster and for patients older than age 50 years with zoster of any severity. Most authors on the subject do not advocate the use of antiviral therapy for immunocompetent patients who are younger than 50 years of age and who have mild acute symptoms.
If available, polymerase chain reaction (PCR) techniques are the most sensitive and specific diagnostic tests for detecting the varicella DNA in fluid taken from the vesicles. The direct immunofluorescence antigen-staining test provides an alternative diagnostic modality when PCR is not available, but it carries a lower sensitivity (77% to 82% vs. 94% to 95% with PCR) and a lower specificity (70% to 76% vs. 100% with PCR).
Herpes zoster affects 10% to 20% of the U.S. population. It results from reactivation of latent herpes varicella-zoster (chickenpox) virus residing in dorsal root or cranial nerve ganglion cells. The virus migrates peripherally along axons into the skin. Two thirds of the patients are older than 40 years of age. Herpes zoster is contagious to those who have not had varicella or have not received the varicella vaccine. Although shingles is not as contagious as chickenpox, it can be transmitted by contact with secretions from the vesicles. A patient with zoster can give chickenpox to a susceptible individual. A patient with chickenpox cannot give any other patient herpes zoster.
In addition to increasing age, other risk factors for reactivation of varicella zoster virus include conditions in which there is altered cell-mediated immunity, including diabetes, cancer, administration of immunosuppressive drugs (including corticosteroids), HIV, and organ transplantation. In immunocompetent patients, zoster is usually a self-limiting localized disease and heals within 3 to 4 weeks. Most patients can be reassured that their disease will abate without permanent problems. The incidence in immunocompromised patients is up to 10 times higher than in immunocompetent hosts, and usually their treatment must be more aggressive.
In these immunocompromised patients, herpes zoster can become disseminated, with lesions appearing outside the primary dermatomes and with visceral involvement. These patients generally require hospital admission for IV antiviral therapy.
The most common complication of herpes zoster is postherpetic neuralgia (i.e., pain along cutaneous nerves, persisting more than 30 days after the lesions have healed). This is more likely to occur in older patients (60 years of age or older), those in whom the degree of skin surface involved is larger, and those with severe pain at time of presentation. Both the incidence and the duration of postherpetic neuralgia are directly correlated with the patient’s age; nearly half of patients 60 years of age or older will develop enduring neuropathic pain. Pain can persist for months and in some patients for many years and can be the source of debilitating neuropathic pain, with considerable physical and psychosocial morbidity.
The tricyclic antidepressant amitriptyline (Elavil) can be used to treat such pain. It can be started at 12.5 to 25 mg daily and increased by 12.5 to 25 mg every 3 to 5 days, to a maximum of 250 mg daily. The most common side effects are dry mouth, constipation, and sedation, which are generally not a major problem at the relatively low doses needed for effect (average dosage being 70 mg daily).
At present, the most promising analgesic approaches for reducing the risk for postherpetic neuralgia, beyond that achieved by antiviral agents, is treatment with an opioid analgesic or with one of the anticonvulsant drugs, such as gabapentin (Neurontin) and pregabalin (Lyrica). These are drugs that already have demonstrated efficacy in treating postherpetic neuralgia (PHN).
PHN can be treated with oxycodone (Oxycontin), titrating the dosage from 10 mg bid to effect or a maximum of 60 mg bid or until the patient experiences intolerable side effects. Common side effects include constipation, sedation, and nausea.
The anticonvulsant gabapentin is an alternative choice for treating PHN. The dosage can be started at 300 mg daily divided tid and titrated over 2 weeks to a maximum of 1800 mg daily divided tid (although dosages up to 3600 mg have been used). Side effects include sedation and dizziness. Pregabalin can also be used, initially starting with 75 mg bid and increasing within 1 week to 100 to 150 mg bid. Always take into consideration that dosage is to be adjusted to a patient’s medical history and tolerance.
Intrathecal methylprednisolone is an option for PHN patients with persistent pain.
It is interesting that most immunosuppressed individuals who develop zoster, even those with disseminated disease, do not develop PHN.
The new live attenuated varicella-zoster vaccine (Zostavax), which is a more powerful version of the vaccine currently given to children for chickenpox, is approved for adults age 60 years and older. It is expected to reduce the incidence of herpes zoster by about 50% and greatly reduce the severity and duration of the disease in those cases that do occur after vaccination. Its efficacy overall in preventing postherpetic neuralgia was 67%. The duration of protection and the need for booster vaccination remain to be determined.

Full access? Get Clinical Tree


