Hemodynamics and Neuroimaging of Migraines
Margarita Sanchez del Rio
Jes Olesen
Hans-Christoph Diener
The study of vascular mechanisms of migraine falls into three epochs: Throughout the nineteenth century and the first half of the twentieth century, studies emphasized the pulsating nature of headache, the existence of vasodilator-induced headaches, and the efficacy of vasoconstrictor agents in the treatments of migraine (45). The group of Harold G. Wolff (61) utilized available primitive techniques with ingenuity to collect evidence for the vascular nature of migraine and formulated what was for decades the textbook concept of migraine mechanisms. The aura symptoms were thought to be secondary to vasoconstriction-induced cerebral ischemia and the headache secondary to reactive hyperemia. The second epoch came with the possibility of measuring regional cerebral blood flow (rCBF) quantitatively and the demonstration of altered rCBF during attacks. The rCBF pattern was shown to be much more complicated than previously thought and incompatible with spasm of major arteries as the initiating event (38). Olesen has reviewed the circulatory mechanisms of migraine and other headaches as of 1991 (35). The reader is referred to this source and another for review of the older evidence (36); therefore, only the best of the older studies is cited in the present text. The third and present epoch uses techniques with a high spatial (positron emission tomography [PET] and magnetic resonance [MR]) and temporal (transcranial Doppler [TCD] and MR) resolution. Metabolism, diffusion, and receptor binding can be measured using PET and functional MR imaging (fMRI), and brain arteries can be depicted accurately and noninvasively by MR angiography.
BRAIN BLOOD FLOW CHANGES IN MIGRAINE WITH AURA
Interictal Studies
Most (1,28,38,42) but not all (12) studies of rCBF using 133-Xenon (133Xe) inhalation with stationary detectors or single-photon computed tomography (SPECT) found interictal absolute flow as well as the flow pattern to be normal. Lauritzen and Olesen (27) found one case with persistent rCBF asymmetry despite normal CT. Also, other studies indicated the existence of asymmetries (30). In juvenile patients, persistent asymmetries were described in 4 of 20 patients (53).
Several of these studies can be criticized for one or more methodologic features, such as the representativity of the case material, statistical methods, possibility of mass significance as a result of regions of interest defined post hoc or of multiple comparisons, lack of partial pressure of carbon dioxide (PCO2) control or influence from extracerebral tissues. The largest study, however, which used a brain-dedicated SPECT system, found significant asymmetries (15) that could not be related to the clinical symptoms. On balance, an interictal mild dysregulation of rCBF is possibly present interictally in migraine with aura.
TRIGGERING OF ATTACKS BY ANGIOGRAPHY
Of 54 patients with aura symptoms involving the extremities, 16 developed their typical aura symptoms following angiography after a lag phase of 0.5 to 1 hours (25). In four cases, vertebral angiography was performed without any migraine reaction. Induced and spontaneous attacks were similar. Olesen and his group observed the same in subsequent rCBF series (28,37,38,39). Mechanisms of migraine induction are uncertain. Disruption of the blood-brain barrier resulting from hypertonic contrast was favored by Janzen et al. (25), who observed spasm of a major cerebral artery in only four patients, two failing to develop migraine attacks. Skinhoj (47) and Skinhoj and Paulson (48) studied intracarotid rCBF followed by carotid angiography. At the height of aura symptoms and rCBF reduction, angiography was normal except for filling of the top of the basilar
artery through the circle of Willis, which could be caused by increased vascular resistance in the carotid distribution. Spasm is therefore an unlikely mechanism, but there are several other possibilities: an irritative effect of contrast materials on the arterial endothelium, cold temperature of the injectate, the passage of non-oxygen-carrying contrast material, pressure from the injection distending the artery, or simple mechanical irritation of a neural puncture or a catheter tip in the artery. We favor the idea of forcible distention of the internal carotid artery by injection inducing activity in perivascular nerves and an arterial-arteriolar reflex response, which in return may cause focal flow reduction, thereby triggering cortical spreading depression (vide infra).
artery through the circle of Willis, which could be caused by increased vascular resistance in the carotid distribution. Spasm is therefore an unlikely mechanism, but there are several other possibilities: an irritative effect of contrast materials on the arterial endothelium, cold temperature of the injectate, the passage of non-oxygen-carrying contrast material, pressure from the injection distending the artery, or simple mechanical irritation of a neural puncture or a catheter tip in the artery. We favor the idea of forcible distention of the internal carotid artery by injection inducing activity in perivascular nerves and an arterial-arteriolar reflex response, which in return may cause focal flow reduction, thereby triggering cortical spreading depression (vide infra).
rCBF IN THE EARLY PHASE OF THE ATTACK (INDUCED ATTACKS)
In the great majority of cases, the first observed event has been a reduction of brain blood flow at the posterior pole of the brain (Fig. 37.1) (18,27,28,34,37, 38, 39,41,42,49). Focal as well as global reductions in rCBF have been reported, but investigations that used equipment with a high spatial resolution all showed a focal start for the reduction in rCBF (see Fig. 37.1). This finding was first made clear in the study of Olesen et al. (38) and was confirmed by Lauritzen et al. (28) and Skyhoj Olsen et al. (49). Each of the 254 detectors in this camera measured rCBF in an area of approximately 1 cm2 of the cortical mantle of the brain. Using this method it is possible to measure rCBF in the same patient up to 10 times at 5- to 10-minute intervals. Measurements were obtained during the pre-aura, the aura, and in some cases the headache phase (18,28,37,38,49). The first abnormality observed was focal hyperperfusion followed by hypoperfusion in three of six patients by Olesen et al. (38), in two of three cases by Friberg et al. (18), although not by other authors. Verification of this preceding hyperemia has been possible with fMRI, being immediately followed by hypoperfusion (21). The subsequent low-flow region usually expanded from the posterior pole of the brain into parietal-occipital-temporal regions and occasionally the whole hemisphere (see Fig. 37-1) (28,38).
A focal low-flow region may appear occasionally in the central part of the frontal region, perhaps because the posterior hypoperfusion has spread through the insula into the frontal lobe, sparing the primary sensorimotor cortex (28) (see Fig. 37-1). The frontal hypoperfusion, again, spreads gradually in all directions, approximately 2 mm/min, so that occasionally all of the frontal lobe becomes affected. Friberg et al. (18) described three cases in which migraine aura, not involving visual symptoms, was associated primarily with frontal lobe hypoperfusion that gradually enlarged and spread posteriorly to involve precentral and post central regions. This gradual enlargement of the low-flow area was termed spreading oligemia by Olesen et al. (38). Spreading hypoperfusion may be, however, a more encompassing term and is used herein. The initial calculations estimated progression at approximately 2 to 3 mm/min in the posterior to anterior direction (28) (see Fig. 37-1), a read score proved inaccurate because the cerebral cortex is convoluted and the observations were few. More recent blood flow measurements performed with blood oxygen level-dependent (BOLD-fMRI) flattening and a computed program surface that permitted more precise measurements of the spread of the hypoperfusion of 3 to 5mm/min, well within the range of experimental cortical spreading depression (CSD) (21).
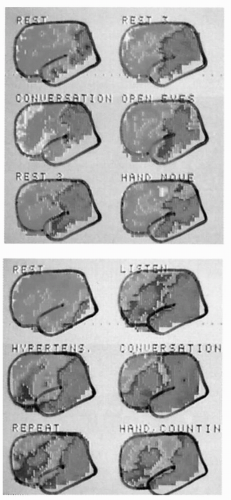 FIGURE 37-1. Original flow results from patients studied before and during the development of a migraine attack with aura. Note the gradual spread of hypoperfusion and the seemingly independent focus in the frontal lobe. There is lack of functional activation in the focal area. (From Lauritzen M, Olesen J. Regional cerebral blood flow during migraine attacks by Xenon-133 inhalation and emission tomography. Brain. 1984;107:447-461.) |
Woods et al. (61) reported changes of rCBF in a woman with the start of an unexpected spontaneous migraine attack while participating in a visual activation study. After the sixth scan, she developed unilateral headache, nausea, photophobia, and phonophobia. The visual activation paradigm was stopped and rCBF was analyzed while the patient kept her eyes closed during the next six scans. The first decrease in rCBF, noted during the seventh scan, was found bilaterally in the visual association cortex. In each subsequent scan, every 12 minutes, the decrease in rCBF spread forward across the cortical surface toward parietal and occipitotemporal areas at a relatively constant rate, sparing the cerebellum, basal ganglia, and thalamus. The authors estimated the maximal decrease of rCBF (oligemia) to be about 40%. Most of these changes, however, were of relatively short duration, with substantial recovery by the time of the next measurement 12 to 15 minutes later.
This case report illustrated for the first time, using PET, a bilateral spreading hypoperfusion in a spontaneous migraine attack in a human subject. Even more remarkable was the patient described only vague visual disturbances not fulfilling diagnostic criteria for visual aura. The measurements could indicate that “subclinical” spreading oligemia occurs in migraine without aura, not reaching the threshold for perceptual deficits. Typical hyperperfusion in the advance of spreading depression known from animal experiments was not detected in this patient, possibly because of relatively poor spatial and temporal resolution (integration over 90 seconds) of rCBF measurements with PET. Also, changes were short lasting, with substantial recovery over a relatively short time, so that delayed measurements might not detect it.
After the slow spread of hypoperfusion, rCBF usually remains unchanged for at least 0.5 to 2.5 hours. In SPECT studies, rCBF reduction virtually always has been posterior, involving a smaller or larger part of one hemisphere. With SPECT, typical blood flow abnormalities were mostly in patients who experienced both visual and sensory auras, less frequently in patients with pure visual auras. This is probably owing to technical factors because marked changes were observed with perfusion-weighted MR in pure spontaneous visual aura (8).
In patients with typical aura, that is, slow march of visual and sensory symptoms, flow reduction is almost inaccurate, whereas less typical aura symptoms, such as diffuse hazy vision or spots, were associated usually with normal rCBF (unpublished results); the case of Woods et al. (61) is an exception.
Completely “out of tune” with others are the findings by Andersson et al. (2) of normal cerebral metabolic rate glucose in induced attacks of migraine with aura; differences in classification or differences in technical features may be responsible for the lack of positive findings.
rCBF IN THE EARLY PHASE OF SPONTANEOUS MIGRAINE AURA
Perfusion-weighted imaging (PWI) provides estimates of hemodynamic changes based on the signal loss caused by the first pass of a bolus injection of a paramagnetic contrast agent through the brain parenchyma. This technique permits multiple measurements during the migraine attack without the need of a radioactive tracer. Three parameters—rCBf, regional cerebral blood flow volume (rCBV), and mean transit time (MTT)—are obtained in approximately 1 minute. The total dose of contrast media (0.4 mmol/kg) and the interval between injections (30 minutes owing to the plasma Gd-DTPA half-life of 20 to 40 minutes) determine the number of measurements within a limited period of time. Such minimal technical requirements have permitted the study of spontaneous cases of migraine with pure visual aura (8,44). Seven spontaneous visual auras in six patients were imaged as early as 20 minutes into the attack as well as seven headache phases after aura in three patients. There was a 27% (14 to 35%) and 15% (2 to 33%) decrement in rCBF and rCBV, respectively, and an increase in the MTT of 32 ± 0.3%, in occipital cortex contralateral to the affected hemifield. Hemodynamic changes persisted up to 2.5 hours into the headache phase. Other brain regions failed to show significant perfusion changes. In one patient who experienced both migraine with and without aura, perfusion deficits were observed only during aura; hemodynamic changes in occipital lobe appear to be a useful marker of migraine with visual aura. Study of spontaneous cases of migraine aura with a technique not subject to Compton scatter has verified the previous findings in induced attacks.
MIGRAINE AURA AS A CLINICAL MANIFESTATION OF CORTICAL SPREADING DEPRESSION
A possible relationship of CSD to migraine aura was already pointed out by Leao and discussed extensively by Lauritzen (26). Spread of first aura symptoms and spread of CSD are at the same speed. Also, the spread of consequent hypoperfusion propagates at a similar speed (28). Recently using fMRI-BOLD, with high temporal and spatial resolution, multiple neurovascular characteristics of CSD (Table 37-1) were demonstrated within the same attack of migraine visual aura (21); five attacks of stereotypical migraine visual aura were studied in three patients. Time-locked to the onset of the visual percept, there was an initial cortical hyperemia lasting 3.3 ± 1.9 minutes, marching across the cortex at a rate of 3.5 ± 1.1 mm/min. This hyperemia, likely the correlate of flashing, jagged lights described during aura is followed by a wave of
hypoperfusion crossing vascular boundaries of contiguous cortex (Fig. 37-2). Although hyperemia is the response to increased neuronal activation, hypoperfusion reflects depressed neuronal function, still clearly present when headache starts. With the aid of cortical flattening and retinotopic techniques, area V3A was determined as the first to develop BOLD signal changes in two attacks of the same subject. Such extrastriate foci are consistent with prior reports (61). Area V3A is especially sensitive to both motion and luminance contrast (57); aberrant neuronal firing in this location might well produce scintillations like those described by migraineurs during a typical visual aura. Moreover, area V3A is retinotopic, with continuous representation of a whole hemifield, again consistent with the progression of a typical migraine aura.
hypoperfusion crossing vascular boundaries of contiguous cortex (Fig. 37-2). Although hyperemia is the response to increased neuronal activation, hypoperfusion reflects depressed neuronal function, still clearly present when headache starts. With the aid of cortical flattening and retinotopic techniques, area V3A was determined as the first to develop BOLD signal changes in two attacks of the same subject. Such extrastriate foci are consistent with prior reports (61). Area V3A is especially sensitive to both motion and luminance contrast (57); aberrant neuronal firing in this location might well produce scintillations like those described by migraineurs during a typical visual aura. Moreover, area V3A is retinotopic, with continuous representation of a whole hemifield, again consistent with the progression of a typical migraine aura.
TABLE 37-1 Comparison of Migraine with Aura and Leao’s Spreading Depression (SD)
Related posts:
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
|---|





