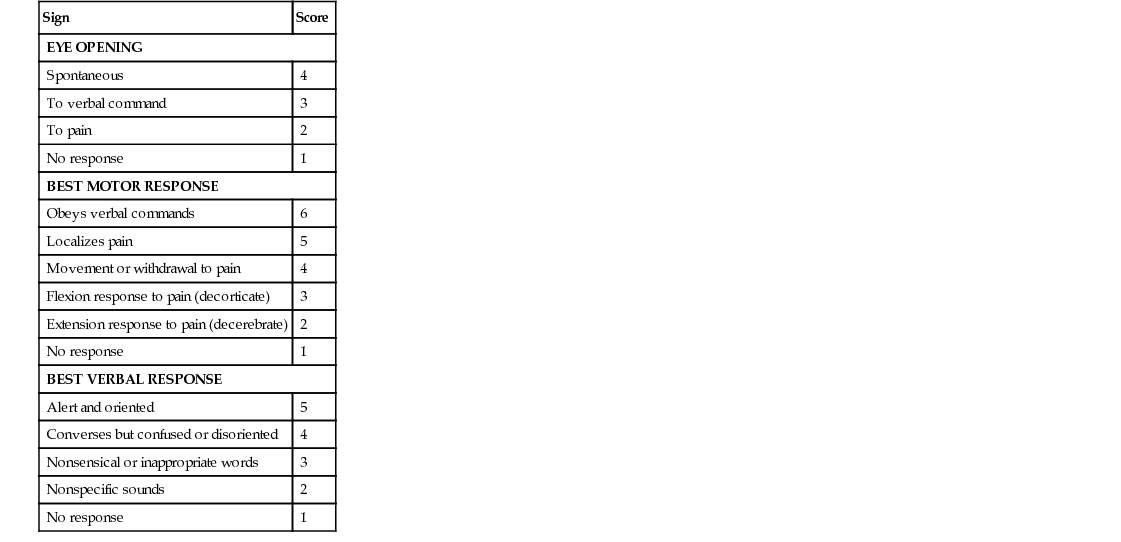
Terry Mahan Buttaro Each year, up to 2.5 million people in the United States sustain a traumatic brain injury (TBI).1 This number can be deceiving, however, because many individuals who incur a sports or recreational brain injury are not hospitalized, nor do they seek emergency department treatment.2 Falls are the number one cause of TBI in children younger than age 14 and in adults older than age 65.1 Unintentional blunt trauma and motor vehicle accidents are the second and third most common causes of TBI with motor vehicle crashes the second most common cause of TBI death.1 Older adults require more hospitalizations and have a higher mortality rate than other age groups for TBI. In elders, morbidity and mortality are related to an increased fall risk as well as increased brain tissue fragility and age-related changes.3 The costs nationwide are significant: 76.5 billion dollars per year.1 TBI is also a common injury for active duty military personnel and can range from mild to severe depending on the type of injury.4 There is increased concern about the number of mild traumatic brain injuries (MTBIs) and undiagnosed TBIs that occur not only in combat but also in sports and recreational activities.2 In MTBI, imaging studies may be normal, but patients may complain of a variety of symptoms that affect daily work and life activities for weeks to months after the injury.2 Repetitive brain trauma or chronic traumatic encephalopathy is usually related to repeated injuries and is often associated with sports. Although chronic head trauma does not result in immediate death, there are chronic brain changes that cause depression and other personality changes, as well as Alzheimer or Parkinson disease.2 The injury can be mild or severe enough to dramatically affect a patient’s intellectual and physical capacity as well as his or her psychological, social, and economic well-being. Loss of consciousness has always been considered one of the most significant indicators of brain injury.5 However, patients with MTBI may not lose consciousness, and patients with epidural bleeding may have only brief loss of consciousness, then be alert and behave appropriately before clinical deterioration rapidly ensues.2 It is essential that health care providers be aware of the “talk and deteriorate” syndrome. Patients with this syndrome utter recognizable words after the head injury and then deteriorate to a severe, brain-injured condition within 48 hours. The most common neurologic findings are altered mental status and focal hemispheric deficits. For these patients, early and appropriate use of computed tomography (CT) scanning is helpful in detecting significant intracranial lesions before clinical neurologic deterioration occurs. Older patients can also incur serious injury even when the head injury is minor. In general, however, patients who lose consciousness for more than 10 minutes or have a focal neurologic deficit are considered to have a major brain injury, whereas those who are unconscious for less than 10 minutes and have no neurologic deficit are classified as having a minor TBI.3 In acute injury, the severity of damage can be described by an injury-rating system such as the Glasgow Coma Scale (GCS) score (Table 32-1).6 The GCS assesses eye opening responses, motor responses, and verbal responses. Numbers are assigned for the level of function attained in each category and then totaled. A normal patient has a score of 15, whereas a patient who is brain dead has a score of 3. Minor head trauma is defined as an initial GCS score of 13 to 15 and a period of unconsciousness of less than 20 minutes. Moderate head injury refers to an initial GCS score of 9 to 12 with or without loss of consciousness. Severe head trauma is defined as an initial GCS score of less than 8 or a comatose state for 6 hours or more.6 The cranial vault is a fixed space that contains the brain, cerebrospinal fluid (CSF), and blood. Because the skull limits intracranial volume, neurologic damage after head injury can be directly related to cerebral edema that causes increased intracranial pressure (ICP), which in turn decreases cerebral blood flow and causes cerebral ischemia. Head trauma can consist of soft tissue injury, skull fracture, and/or hemorrhage. Brain injury from trauma can occur in two stages: primary and secondary. Primary injury is sustained in the initial insult and may result from blunt trauma, penetrating injury, coup-contrecoup lacerations or contusions of the brain, or direct disruption of brain tissue by the shearing of axons. Secondary injury may occur from increased ICP, cerebral hypoxia, systemic hypotension, decreased cerebral blood flow, and oxygen free radicals resulting in cellular death. The secondary sequelae may cause further neuronal damage, which can compromise an already injured brain. In mild TBI, the primary cause of injury is the dysfunction of brain metabolism rather than structural injury.7 It is important to establish the mechanism of the trauma, the stability or progression of the patient’s symptoms, the patient’s prior condition, and the patient’s significant medical history including current medications (especially antiplatelet or anticoagulant therapy) and allergies. The cause and exact location of the injury should be determined: Was it accidental or intentional? Changes in mentation and any loss or change in level of consciousness should be determined and elicited not only from the patient, when possible, but also from witnesses. A history of amnesia (retrograde or anterograde) concerning the traumatic event, even if fleeting, often indicates altered consciousness and needs to be quantified.2 It is also necessary to ascertain consciousness before the head injury to identify other pathologic conditions, such as stroke, myocardial infarction, or respiratory distress. Additional causes of altered mental status, such as hypoglycemia, drug overdose, hyperthermia, or arrhythmias, must also be investigated. Alcohol intoxication can mask the signs and symptoms of a head injury; therefore it is important to determine if alcohol was involved. The history should also elicit previous history of concussion or other brain trauma, complaints of seizure activity, confusion, drowsiness, dizziness, headache, visual changes, blurred vision, tinnitus, slurred speech, neck pain, nausea, vomiting, upper or lower extremity weakness, difficulty concentrating, and emotional lability such as increased irritability or other change in behavior.2 In older patients, the first sign of brain injury may be confusion or a change in behavior rather than a reported fall or other injury. The patient may not remember a fall or injury or may believe that the injury was insignificant. Family members or caregivers may also not be aware that an event occurred.
Head Trauma
Definition and Epidemiology
Pathophysiology
Clinical Presentation



Full access? Get Clinical Tree


