Figure 18.1. Cutaneous innervation of the head and face. The posterior half of the head is innervated by branches from the dorsal rami of the C2 spinal nerves. The face and anterior half of the head are innervated by divisions of the fifth cranial nerve (V1, V2, V3). Terminal cutaneous branches of V1 include supratrochlear, supraorbital, infratrochlear, external nasal, and lacrimal. Terminal cutaneous branches of V2 include zygomaticotemporal, zygomaticofacial, auriculotemporal, and infraorbital. Terminal cutaneous branches of V3 include mental and buccal (generally blocked intraorally).
1. Ophthalmic nerve (V1). The ophthalmic nerve is the smallest and most superior of the three trigeminal divisions. Its branches enter the orbit to supply a variety of intraorbital and extraorbital structures associated with the eye. The only branches that have a significant extraorbital course, and are therefore readily amenable to nerve block, are the supraorbital and supratrochlear branches.
a. Supraorbital nerve. The supraorbital nerve exits the orbit through the supraorbital notch, which is located near the middle of the supraorbital rim directly above the pupil when looking straight ahead (Figure 18.3). The supraorbital nerve supplies the upper eyelid, forehead, and scalp to the vertex (Figures 18.1, 18.2, and 18.3).
b. Supratrochlear nerve. The supratrochlear nerve emerges from the upper, medial quadrant of the orbit and courses superiorly across the orbital rim. The supratrochlear nerve innervates the medial portion of the upper lid and the medial portion of the lower forehead (Figures 18.1, 18.2, and 18.3).
2. Maxillary nerve (V2). The maxillary nerve exits the cranial vault through the foramen rotundum to cross through the pterygopalatine fossa, which lies between the pterygoid plate and the posterior border of the maxilla (Figures 18.2 and 18.4). Within the fossa, the maxillary nerve gives off several branches that provide sensory innervation to the maxilla, maxillary sinus, nasal canal, palate, and the skin over the temple and zygomatic arch. The nerve continues forward and enters the orbit through the infraorbital canal, pierces the orbital floor to traverse the maxillary sinus (this is why maxillary sinusitis can present as cheek pain) and exits the maxilla as the infraorbital nerve.
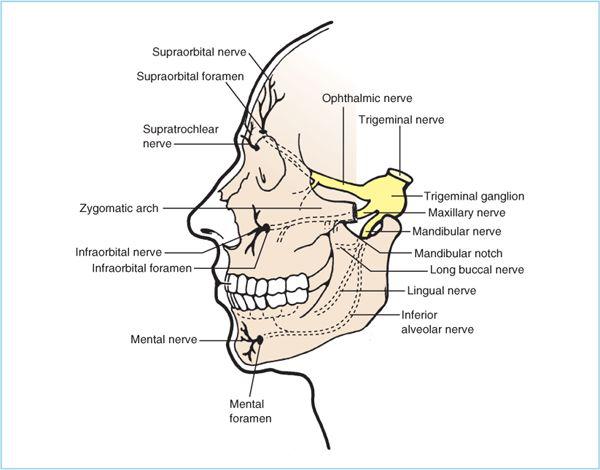
Figure 18.2. Anatomy of the trigeminal nerve, trigeminal ganglion, and primary divisions of the trigeminal nerve. Only the terminal branches of the ophthalmic nerve are accessible for extracranial blockade. In contrast, the maxillary and mandibular nerves can be blocked at multiple points along their course from the lateral pterygoid plate to the terminal branches exiting the infraorbital and mental foramina.
a. Infraorbital nerve. The infraorbital nerve exits the maxilla through the infraorbital foramen, which lies just below the infraorbital rim in line with the pupil when looking straight ahead (Figure 18.3). The infraorbital nerve provides sensory innervation to the cheek, the lower eyelid, the nasal ala, and the upper lip.
b. Zygomatic nerve. The skin over the zygomatic arch and the temple are innervated by the zygomatic and zygomaticotemporal nerves, respectively. These branches of the maxillary nerve arise in the pterygopalatine fossa (Figure 18.4); consequently, block of the infraorbital and supraorbital nerves will leave this area of the facial skin unblocked (compare Figures 18.1 and 18.3).
3. Mandibular nerve. The mandibular nerve is the largest of the three trigeminal branches and is the only one with motor fibers. It exits the cranial vault through the foramen ovale, which lies in the sphenoid bone just posterior to the origin of the pterygoid plate (Figure 18.4). After exiting the foramen ovale, the mandibular nerve gives several branches to muscles in the pterygoid fossa and muscles of mastication (masseter, temporalis). Sensory fibers include:
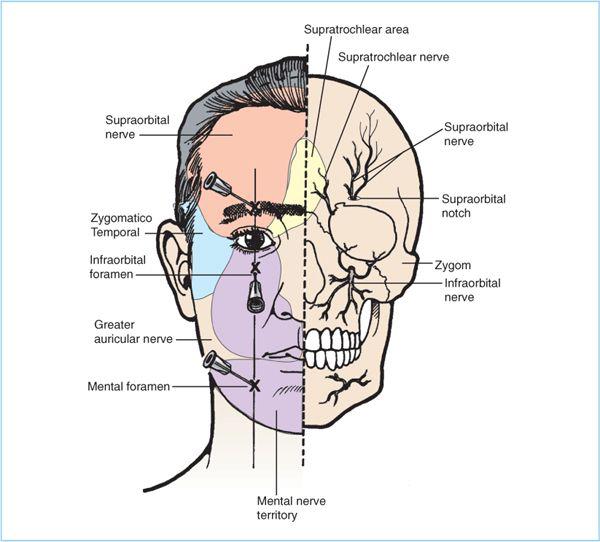
Figure 18.3. Cutaneous innervation of the face. Most of the face and forehead are innervated by the terminal branches of the ophthalmic (supraorbital, supratrochlear), maxillary (infraorbital), and mandibular (mental) nerves. The foramina through which the supraorbital, infraorbital, and mental nerves emerge lie along a straight line passing through the pupil when the subject looks straight ahead.
a. Auriculotemporal nerve. The auriculotemporal nerve courses medial to the condylar process of the mandible and turns superiorly at the posterior border of the process becoming superficial near the posterior part of the zygomatic arch (Figure 18.4). It runs superiorly providing sensory innervation to the anterior half of the ear, the skin anterior to the ear and the skin over temporalis muscle.
b. Inferior alveolar nerve. As the mandibular nerve courses inferiorly within the pterygopalatine fossa it divides into two main branches–inferior alveolar and lingual (Figure 18.4). The inferior alveolar nerve descends parallel to the ramus of the mandible to enter the mandible through the mandibular foramen, which lies at approximately the center of the ramus (Figure 18.2). The inferior alveolar nerve provides innervation to the buccal gingiva, mandible, and lower teeth.
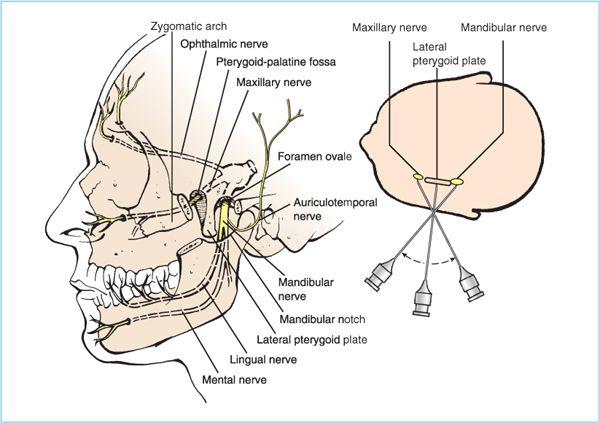
Figure 18.4. Lateral approach to the maxillary and mandibular nerves. For both mandibular and maxillary nerve blocks the needle is inserted through the mandibular notch to contact the lateral pterygoid plate. For maxillary nerve block, the needle is walked anteriorly off the pterygoid plate and into the pterygopalatine fosse where 5 mL local anesthetic is injected. For mandibular nerve block the needle is walked posteriorly off the lateral pterygoid plate. See text for details.







Full access? Get Clinical Tree


