Handle Dental Injuries as You Handle Teeth, With Care
Douglas W. Anderson DMD
Kenneth R. Abbey MD, JD
Your first patient of the day is a middle-aged, morbidly obese man having an inguinal hernia repair, who happens to have the brightest, whitest smile you have ever seen. During his preoperative interview, he mentions that he used to have terrible teeth but has recently had a “major makeover” including the “caps” that give him his great smile. Of course, he turns out to be a difficult intubation; and while you are sneaking that bougie under an epiglottis you can only see the tip of, you hear the sharp crack of his front caps giving way to your Mac 4.
Injury to the teeth before anesthesia, during induction of or emergence from anesthesia, or under sedation is not common. Nevertheless, such injuries represent the single largest source of claims against anesthesia providers. The average payment for dental injury is only $1,700. However, because dental injuries constitute 29% of claims, total indemnity payments are substantial. In addition, administrative expenses associated with verifying and paying the claims add significantly to the cost.
Management of dental injuries begins before they occur. The first task for the anesthesia provider is to have a working knowledge of how dental injuries are handled in their institution. Be aware that there is a wide range out there! The editor has provided anesthesia care in hospital systems with policies that have ranged from providing no reimbursement for the repair of dental damage (on the advice of the institution’s legal department, who feel that would represent a tacit admission of malpractice) to essentially providing free dental care for life. The second task for the anesthesia provider is to have a basic knowledge of dentition (if you can memorize the branches of the brachial plexus, you can master the simple numbering system of the teeth, Fig. 187.1). The third part of managing dental injuries before they happen involves discussion and documentation. Junior anesthesia providers who have never been involved in a dental complication often do not carefully document the exam of the teeth, whereas more experienced anesthesiologists and anesthetists who have seen complications do! Look closely at the teeth and take a minute to jot down the number of teeth that are missing or hanging by a thread (sometimes, it is more expedient to note where there are teeth, instead of where there aren’t teeth). Also take notice of any open or fresh
sockets. This documentation can seem costly in terms of time, and junior anesthesia providers are sometimes resistant to doing it. But consider the time required to bronch the patient while you are standing there thinking, “Did we bump that out, or was that the tooth the patient said fell out last night?”
sockets. This documentation can seem costly in terms of time, and junior anesthesia providers are sometimes resistant to doing it. But consider the time required to bronch the patient while you are standing there thinking, “Did we bump that out, or was that the tooth the patient said fell out last night?”
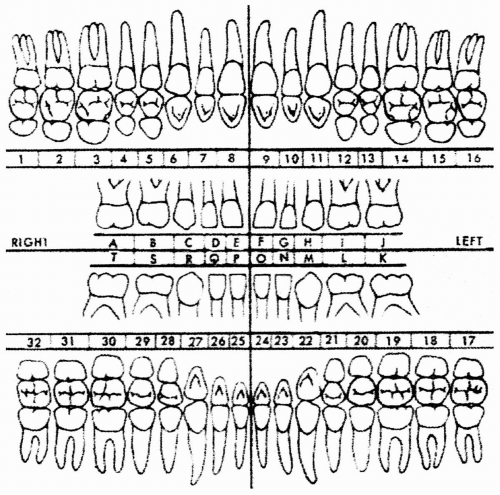 FIGURE 187.1. Number system of the teeth. (From McDonald RE, Avery DR. Dentistry for the Child and Adolescence. 3rd ed, St. Louis: Mosby; 1978:5.)
Related posts: Never Neglect the Basics of Airway Management
Consider the Use of Lidocaine in the Cuff of the Endotracheal Tube, But Be Aware of the Risks and Alternatives
Do Not Underestimate the Difficulty of Reintubating a Patient Who Has Undergone Carotid Endarterectomy or Cervical Spine Surgery
Don’t Overflush Lines
Do Not Treat Lactic Acidosis with Bicarbonate
Beware the Antibiotic Bowel Prep Never Neglect the Basics of Airway Management
Consider the Use of Lidocaine in the Cuff of the Endotracheal Tube, But Be Aware of the Risks and Alternatives
Do Not Underestimate the Difficulty of Reintubating a Patient Who Has Undergone Carotid Endarterectomy or Cervical Spine Surgery
Don’t Overflush Lines
Do Not Treat Lactic Acidosis with Bicarbonate
Beware the Antibiotic Bowel Prep

Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|