Chapter 13
Geriatric Issues and the ICU
Richard M. Bell and Victor Hurth
Chapter Overview
Population ageing with growth rate of nearly 4% per year in those over 80 years of age is a global phenomenon.1 Some studies report that the percentage of patients ≥80-years-old admitted to intensive care unit (ICUs) approaches 15%.1 The ageing process itself reduces physiologic reserve and is frequently referred to as homeostenosis. Those with multiple comorbidities are at even greater risk making admission to the ICU more likely. Although policies for ICU admission are as diverse as are the healthcare systems.2 Resources must be rapidly expanded to meet the health care needs. Some observers predict that ICU admissions in those over 80 will double by 2015, increasing by 6% per year.5 Options for how expensive resources like ICU care will be managed are limited. The solution will probably be some form of rationing of resources, as the expense is unaffordable and unsustainable.
Age with associated comorbidities pose many challenges for the intensivist including risks of major complications, drug-related side effects and interactions, a general decrease in organ function and the ability to metabolize administered pharmacotherapeutic agents, as well as the ability to respond to cardiorespiratory threats, infections, and surgical illness.
In this chapter, we discuss issues specific to the derangements physiology associated with the ageing process and how they impact ICU care, in order to assist the intensivist caring for these patients.
Characteristics of ICU Admissions for the Elderly
The characteristics of elderly patients admitted to ICUs vary widely and so do criteria for admission. These include personal bias, physician perception, resources, patient, and family wishes etc. The decision for admission is influenced by many factors and involves application of many models (Simplified Acute Physiology Score — SAPS, Acute Physiologic and Chronic Health Evaluation — APACHE), concurrent comorbidities (Charlson Index or Elixhauser Index), functional status of the patient (Knaus, McCabe, Karnofsky, EuroScore, Katz scores, or Barthel Index etc.), physician perceptions regarding appropriateness, futility, and societal ethos. Many decisions are based on the doctors’ impression that the patient is “too sick” or “too well” to benefit from ICU admission and/or aggressive care. Patients admitted to Intensive Care in the United States have lower severity of illness scores, higher admissions for cardiac illness, more chronic medical conditions and half the percentage of patients admitted requiring Mechanical Ventilation (MV) than in the United Kingdom,6 Australia, or New Zealand.1 Origin of admission also varies considerably. In the US more ICU admissions are referred by the Emergency Department, while in other countries more admissions come from hospital wards, transfers from other units, or unplanned surgeries.
Outcome following ICU admission for the elderly
Because of the variability described earlier, it is impossible to make generalizations regarding the outcome of elderly patients following ICU admission. Traditionally, ICU mortality has been the endpoint for judging outcome. More recently, surveys of elderly patients suggest that the return to a previous functional state is a strong patient desire and outcome measure.
Most reviews agree that severity of critical illness and diminished preadmission functional status, have a negative impact on ICU and hospital mortality, length of stay, long-term survival, functional status after discharge, and discharge destination. The requirement for mechanical ventilation within 24-hours of admission or renal replacement therapy also appears to negatively impact survival. ICU admissions from chronic care facilities and those with longer ICU stays also have lower survival rates.
The impact of age alone on outcomes is conflicting. It appears that age >75-years may independently predict bad outcome. In-hospital mortality figures range from 25–80% with one to two organ system failures respectively.6 Bagshaw et al.1 reported that the most common reason for ICU admission was for planned surgery and these patient had an ICU and in-hospital mortality of 12% and 25% respectively. More importantly discharge to home occurred in 72% and 57% of patients who had planned surgery were alive at one year compared to 11% who underwent unplanned surgery.7 Quality of life was good with 83% having no cognitive impairment and three quarters having no physical impairment, the perceived quality of life assessments equating with age-matched controls.8
Physiology of senescence and common organ dysfunctions
in the elderly ICU patient and their impact on ICU care
The ageing process can be described simply as the “stiffening” of all organ systems, due to genetics, oxidative free radical, glycation, and other forms of cellular damage that occurs over the lifetime of an individual, including healthy older adults and this is magnified by comorbidities. Understanding these physiologic limitations will improve the intensivist’s ability to appropriately care for the elderly ICU patient.
Many of the changes seen are associated with a chronic, often low-grade inflammatory process that has been termed “inflammaging”. This has been confirmed by a measured increase in serum markers of inflammatory cytokines and a decrease in serum levels of anabolic hormones and inflammatory suppressor cytokines. Strategies that ameliorate inflammation, improve muscle mass, and nutritional status have been shown to improve outcomes, reduce morbidity and mortality, improve the prospect of a return3,4 to independent living by reducing hospital deconditioning, and mitigate the need for discharge to intermediate care or rehabilitation facilities. Conditioning activities, appropriately termed “Pre-habilitation”, are not always possible for those elderly patients acutely admitted to an ICU setting. In addition, the margin for error in treating the older population is extremely narrow. Even trivial perioperative complications are poorly tolerated by the elderly.
Organ System Changes with Ageing
Cardiovascular9
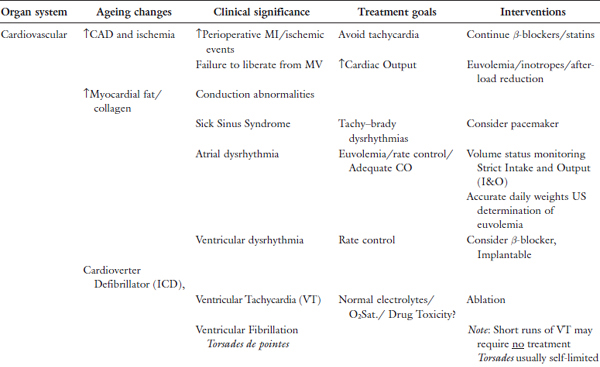
The increasing incidence of Coronary Artery Disease (CAD) and Heart Failure (HF), place the elderly patient at risk for acute cardiac decompensation when in the ICU, Table 1. Response to fluid resuscitation in shock from trauma and other causes and rapid change in fluid dynamics in the perioperative period are quite variable in the elderly and often unpredictable necessitating close central hemodynamic monitoring. Resuscitation often requires inotropes or afterload-reducing agents, unlike their younger counterparts. Many of these patients may have concomitant renal impairment. This, together with the release of ADH and aldosterone in response to stress and surgery make urine output alone an unreliable measure of adequate perfusion. Catecholamine release in response to hypoperfusion states is more likely to result in dysrhythmias leading to poor outcome. Associated coronary artery disease predisposes to acute coronary ischemic events including Myocardial Infarction (MI) and death in response to hypoperfusion states. Patients on β-blockers and antihypertensive agents pose major challenges because the usual blood pressure and heart rate response to hypoperfusion and fluid resuscitation are no longer reliable, again necessitating close central hemodynamic monitoring. In these situations traditional clinical indices of perfusion such as level of consciousness, skin warmth, capillary refill, base deficit, and lack of skin pallor can prove very helpful in addition to central hemodynamic parameters.
Many acute cardiac events may be masked particularly in those over the age of 75. Subtle changes such as clinical decline or failure to wean from mechanical ventilation may be the only indications of ischemic changes. Tachycardia, because of the increase in myocardial oxygen demand versus supply in the face of limited flow due to CAD, may precipitate an acute ischemic event. Withdrawal of chronic β-blockers may result in rebound tachycardia and contribute to reduced coronary blood flow due to a reduction in ventricular filling time during diastole. Diastolic dysfunction (stiffening precluding adequate ventricular filling, common in the elderly) compounds the issue. Tachycardia may also promote coronary arteryplaque rupture leading to infarction. Abrupt discontinuation of statins likewise produces a rebound vascular inflammatory response contributing to reduced coronary blood flow and subsequent thrombosis. Chronic HF may be exacerbated by acute changes in renal function and injudicious fluid administration in the face of the acute inflammatory response as a result of surgical stress or acute illness.
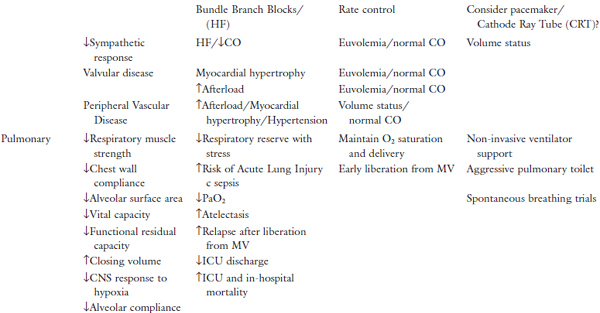
The increase in myocardial fat and collagen associated with ageing results in conduction abnormalities including Atrial Fibrillation (AF) which is the most common. Rate control, usually with β-blockade or a calciumchannel blocker for AF is common. Many elderly patients with chronic AF are anticoagulated with warfarin and more recently with direct thrombin inhibitors and consideration must be given to bridging therapy depending on other treatment considerations and acute medical or surgical issues. Short runs of Ventricular Tachycardia (VT) are usually insignificant and require no treatment. Prolonged VT may prompt the insertion of internal defibrillators. Torsades de points, more common in the elderly, is usually self-limiting, but may precipitate ventricular fibrillation and careful monitoring is mandatory. Bundle branch block, in particular sick sinus syndrome, may require cardiac pacing. Chronic valvular disease such as aortic stenosis most common in the elderly, requires meticulous attention to volume status and occasionally cautious afterload reduction.
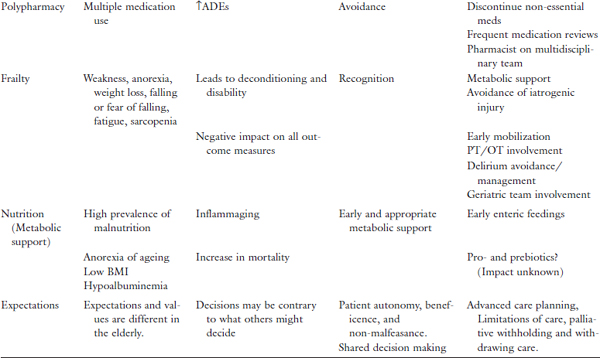
Table 1. Physiologic changes/geriatric issues and impact on ICU care.
Pulmonary10
Ageing results in a decline in all respiratory parameters posing major respiratory challenges in the ICU. Collagen cross-linking results in stiffening of pulmonary parenchyma, increasing the work of breathing, which may necessitate mechanical ventilatory assistance. Frequently this is exacerbated by chronic obstructive and restrictive disease. The tachypneic response to low tidal volume to maintain minute ventilation is frequently misinterpreted as a sign for ventilator dependence.
The known decrease in functional residual capacity and increase in closing volume (see chapter on Perioperative Respiratory Dysfunction) in the elderly which is worse in the supine position leads to alveolar collapse and hypoxemia. Alveolar fibrosis also impairs gas exchange because of ventilation perfusion mismatch. A decrease in responsiveness to hypoxia by the central nervous system results in carbon dioxide (CO2) retention and secondary worsening of the hypoxemia frequently requiring mechanical ventilator support. The risk of acute lung injury also increases in these patients. Relapse after recovery necessitating resumption of mechanical ventilation is also common in these patients.
The elderly also presents many challenges in securing a definitive airway. Bag valve mask ventilation is impeded by inability to obtain a good seal in the edentulous patient, necessitating temporary placement of the patient’s dentures in the mouth to facilitate ventilation. The fragile nasal and oral mucosa may predispose to bleeding during intubation necessitating gentleness. Neck immobility due to kyphoscoliosis and spinal stenosis make visualization of the vocal cords difficult and ancillary airway techniques such as the use of the glide scope, bronchoscope, Laryngeal Mask Airway, and the Gum Elastic Bougie should be made available in anticipation of these difficulties.
Renal11,12
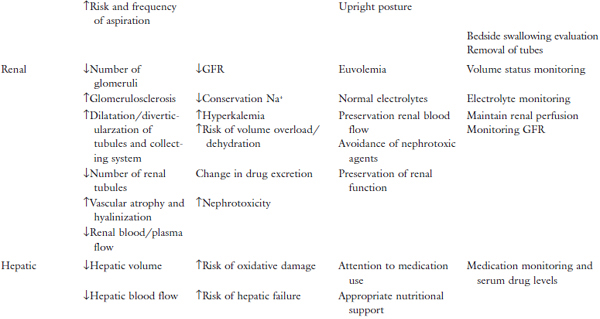
Despite the loss of glomeruli (1/2 to 2/3 of those in younger patients), medullary interstitial fibrosis, glomerular sclerosis, dilatation of the collecting tubules, the reduction in renal blood flow caused by the subendothelial deposition of hyaline, and the reduction in glomerular filtration rate, the ageing kidney is still capable of maintaining homeostasis under normal circumstances. The older kidney is less capable of conserving sodium, perhaps due to lower aldosterone levels and diminished sodium reabsorption. This may be due to a co-existent renin deficiency as the response to Adrenocorticotropic Hormone (ACTH) stimulation is not impaired. The clinical significance is that the elderly do not respond immediately to sodium loading as younger patients do and they tend to develop hyperkalemia on a low sodium diet. The ability to conserve potassium is also restricted in the older patient as evidenced by a 20% reduction in total body potassium. These age related changes predispose the elderly to hyperkalemia particularly in association with acidosis as the aged kidney is slow to respond to the increase in serum hydrogen ion concentrations. Drugs with potential for the inhibition of renal potassium excretion, spironolactone, non-steroidal anti-inflammatory agents, β-blockers, and Angiotensin-Converting-Enzyme (ACE) inhibitors should be used with caution in older patients to avoid the risk of hyperkalemia. Serum levels of calcium are generally lower in the elderly and phosphate levels are higher. In the older patient the response to immobilization is exaggerated producing exceptionally high levels of calcium excretion in the urine. All these changes can be complicated by co-existing renal disease, hypertension, hyperthyroidism, malignancies, and diabetes. Drug dosing and administration must be adjusted in consideration of the changes in the senescent kidney. Many drugs have more direct toxic effects on the kidneys of older adults. These include Nonsteroidal Anti-inflammatory Drugs (NSAIDs), contrast agents used for imaging, aminoglycosides, methotrexate, and many others.
In the presence of renal insufficiency which is common in the elderly, drugs whose clearance is primarily through a renal mechanism should be administered with extreme caution while monitoring serum levels closely. Drugs that are not primarily cleared by renal excretion are preferable. Medications with known nephrotoxicity should be avoided if possible.
Standard estimates of renal function, i.e., serum creatinine and estimates of Glomerular Filtration Rate (GFR) commonly used today, may be misleading in the elderly. This compromises the ability to assess accurately baseline renal function and monitor the change in renal function in critically ill older patients. The Cockcroft–Gault Equation (CGE) is less accurate, overestimating high GFR values and underestimating low values in older patients more so than the Modification of Diet in Renal Disease Formula (MDRDF). Some consider the Chronic Kidney Disease Epidemiology Collaboration formula (CKD-Epi) more accurate. The formulae are provided in Table 2. Considering the changes in creatinine metabolism associated with the loss of muscle mass in older patients, it has been suggested that determination of serum cystatin C alone or in combination with serum creatinine improves the ability to document renal function. Cystatin C is a cysteine proteinase inhibitor produced at a constant rate by all nucleated cells. It is freely filtered by the glomeruli and metabolized in the proximal tubule. Muscle mass and dietary protein intake have little to no effect on the serum levels of this substance. Many formulae have been proposed but unfortunately, the accuracy of using any of these in critically ill patients has not been validated. Further, their use in diabetic patients and the concurrent administration of some medications, e.g., corticosteroids, affect serum levels of this substance, while others interfere with the laboratory analysis.13
Table 2. Formula for estimating GFR in elderly patient.
| Cockcroft–Gault Equation |
|
| Modification of Diet in Renal Disease Formula |
|
| Chronic Kidney Disease Epidemiology Collaborative Formula |
|
| Cystatin C Equation |
|


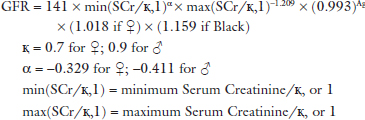

Note: Results of all formula in mL/min/1.73 m2. SCr = serum creatinine; CysC serum cystatin C level.
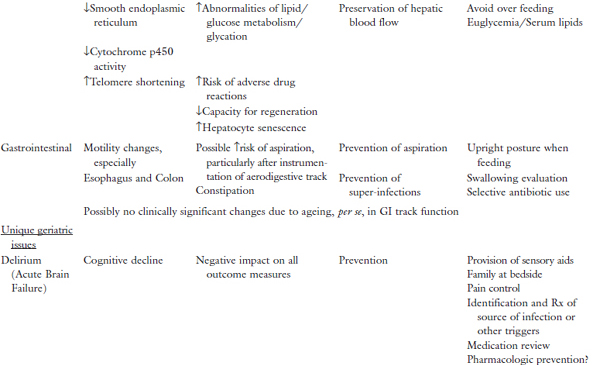
Hepatic14






Full access? Get Clinical Tree


