Immediate Management of Life-Threatening Injuries
Genitourinary injuries occur in 10–20% of major trauma patients. Most of these injuries, with the exception of renal hilar disruption or shattered kidney, are not immediately life-threatening. Because they are often accompanied by potentially life-threatening injuries to other organ systems, however, it is easy for the emergency physician to overlook and therefore miss signs or symptoms of urologic injury. Failure to diagnose and treat these injuries properly can result in significant long-term morbidity. Therefore, while evaluating the trauma patient, the physician needs to be aware of clues to genitourinary injury. These clues include (1) lumbar vertebral or lower rib fractures, (2) pelvic fractures, (3) flank pain or hematoma, (4) abnormal prostate (high riding, nonpalpable, or free floating) on rectal examination, (5) blood at the urethral meatus, and (6) gross hematuria.
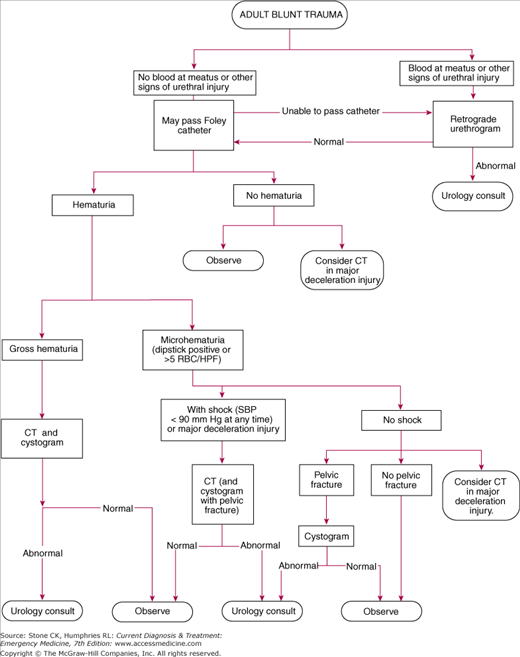
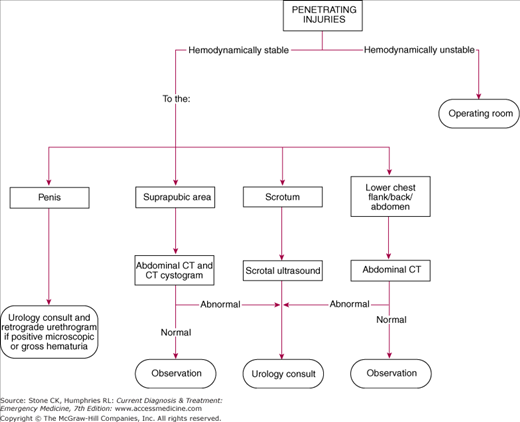
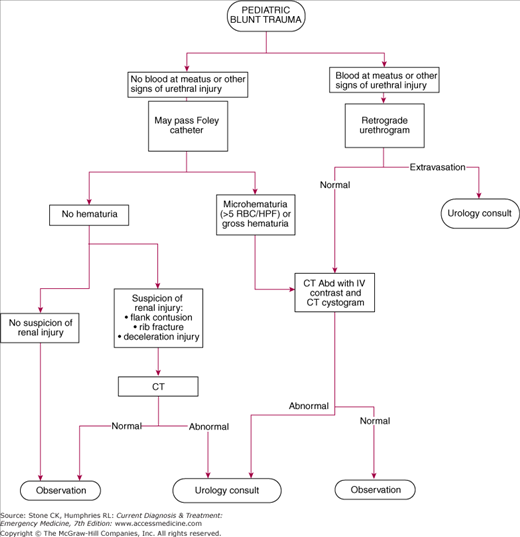
For all patients with blunt or penetrating trauma, evaluate airway, breathing, circulation, and disability during the primary survey as per advanced trauma life support protocol (Chapter 12). During the secondary survey, evaluate for a boggy or high-riding prostate on rectal exam, perineal or scrotal hematoma, and any evidence of blood at the urethral meatus. If any of these signs is present, perform a retrograde urethrogram (RUG) before inserting a Foley catheter. If the signs are absent, insert a Foley catheter if indicated (ie, in unstable patients or those unable to urinate). Urethral studies should never delay diagnostic studies of, or treatment for, potentially life-threatening injuries. Figures 26–1, 26–2, and 26–3 provide algorithms for managing blunt, penetrating, and pediatric urologic injury.
Because of the need to determine if Foley catheter placement is safe, evaluation of the genitourinary system is generally performed in a retrograde fashion: rule out urethral injury before bladder (usually by physical exam), then bladder (by placing a Foley catheter) before ureteral or renal injury.
A Foley catheter may be placed once physical examination supports the integrity of the urethra. As mentioned previously, if any signs of urethral injury are present, perform a RUG first. If the urethrogram is negative or not indicated, a 14–16 F catheter should be placed using copious amounts of lubricating jelly and sterile technique. A folded 4 × 4 in2 gauze pad may be used to retract the foreskin in uncircumcised patients to prevent repeated unintended reduction of the foreskin over the glans with subsequent field and catheter contamination during placement. Any difficulty during placement warrants retrograde urethrography if urethral injury is a possibility. Gross or microscopic hematuria indicates possible urologic trauma, although the degree of microscopic hematuria does not correlate with the degree or location of injury.
In 1989, a 10-year prospective study established guidelines for evaluation and treatment of blunt renal trauma and the consensus opinion remains the same. Patients with gross hematuria require an imaging study. Patients with microscopic hematuria and a history of shock (systolic blood pressure < 90 mm Hg) or sudden deceleration injury should also have an imaging study performed. Those without shock or deceleration injury may be discharged home with outpatient urology follow-up to ensure that microscopic hematuria has cleared. Patients with penetrating injuries and more than 5 red blood cells per high-power field should undergo an imaging study, although the absence of hematuria does not eliminate the need for a study. With regard to penetrating trauma, the location of the wound is more important than the presence of hematuria for predicting injury, because significant injuries (9% of patients in one study) can be present even in the absence of hematuria. In pediatric patients, the kidney is the most commonly injured intra-abdominal organ. Children are more susceptible to renal injuries than adults as their kidneys are proportionally larger and are surrounded by less perirenal fat. The ribcage is also less rigid and does not provide the extent of protection as present in adults. As a result, even microscopic hematuria from trauma requires further workup (usually by computed tomography [CT] scan) in pediatric patients. There is some controversy over the quantity of microscopic hematuria that necessitates further evaluation in children. A review of the current literature yielded varying cutoffs mostly ranging from 5 to 50 RBC/hpf. The authors of one retrospective review even suggested that children should be evaluated in the same manner as adults, which could potentially limit CT radiation. While this topic will likely be subject to future investigation, the current opinion is that pediatric microscopic hematuria in blunt or penetrating trauma should be considered clinically significant and prompt further evaluation.
Suprapubic catheter placement is indicated in trauma situations when Foley catheter placement is contraindicated. This usually occurs in patients with a known or suspected urethral injury who are awaiting a confirmatory study or surgical intervention. Several commercial kits are available. Most of these kits utilize placement over a guidewire. If kits are unavailable, a single-lumen central venous catheter may be used.
Helical CT scan with intravenous contrast is the study of choice for evaluating ureteral or renal trauma. Retroperitoneal structures such as the kidneys, ureters, and bladder are very well visualized by abdominal CT scanning. In the evaluation of renal trauma, CT scanning provides detailed information regarding the extent of hemorrhage, extravasation, and devascularization. The CT scan may also be used for retrograde cystography. Simply clamping the Foley catheter during an intravenous contrast pelvic CT scan is not adequate to eliminate bladder injury, because of inadequate bladder pressures and dilute dye. The technique for this study involves contrast administration into the bladder via the foley catheter.
The RUG is the study of choice to evaluate urethral trauma. If urethral injury is suspected (eg, blood at the meatus, boggy or high-riding prostate, scrotal or perineal hematoma), urethrography should be performed prior to Foley catheter placement. The study is performed by instilling contrast medium into the urethra, usually under fluoroscopy. After a preinjection abdominal X-ray is obtained, a Cooke adapter on a 60-cc syringe is gently inserted into the urethra and approximately 20 cc of water-soluble contrast is injected over 60 seconds. If fluoroscopy is not available, an X-ray is taken during the last 10 seconds of injection. Extravasation with bladder filling denotes partial urethral tear, and extravasation with no bladder filling denotes complete urethral tear.
Similar to the IVP, the retrograde cystogram using plain radiography has essentially been replaced by the CT cystogram. In this technique, up to 400 cc of full-strength water-soluble contrast is instilled under gravity through a urethral catheter to the point of bladder contraction after a preliminary KUB. X-rays are taken with the bladder full and after complete voiding to attempt to visualize extravasation.
Although used frequently in trauma situations to detect peritoneal blood, ultrasound does not have the sensitivity (possibly as low as 22%) to reliably detect specific renal injuries, and therefore is not recommended in the definitive workup of renal trauma.
Mainly mentioned only for historical purposes, the intravenous pyelogram (IVP), which was once the standard of imaging for genitourinary trauma, has been replaced by the helical CT scan due to CT’s superior sensitivity and ability to evaluate for nonurological injuries.
1This chapter is a revision of the chapter by Geoffrey A. Wiss, MD, Claudia Whitaker, MD, & Robert K. Dunne, MD, FACEP from the 5th edition.
Emergency Treatment of Specific Injuries
- Often accompanied by other abdominal injuries in blunt trauma.
- Nausea, vomiting, flank ecchymosis, and lower rib or lumbar fractures suggest injury.
- No reliable markers for diagnosis, including hematuria.
- CT scan is study of choice.
Renal injuries are the most common urologic injuries. The kidneys are not fixed in place but hang from their vascular attachments and perirenal fat and move with the diaphragm. Secured at only the vascular pedicle, the kidneys are susceptible to deceleration injury, with blunt injury five times more common than penetrating injury. Kidneys with preexisting abnormalities such as tumors, congenital lesions, or hydronephrosis may be damaged by seemingly inconsequential mechanisms.
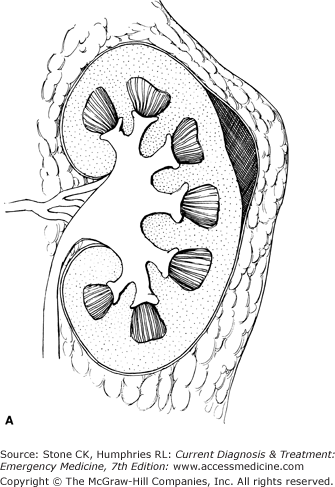
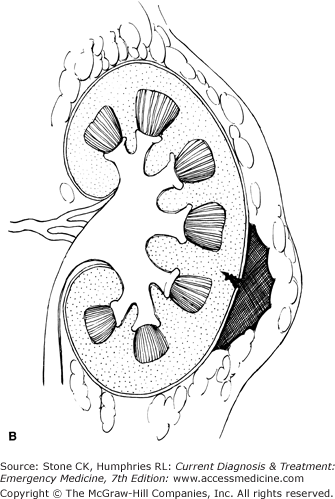
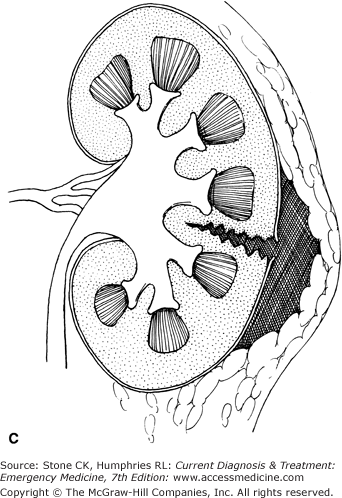
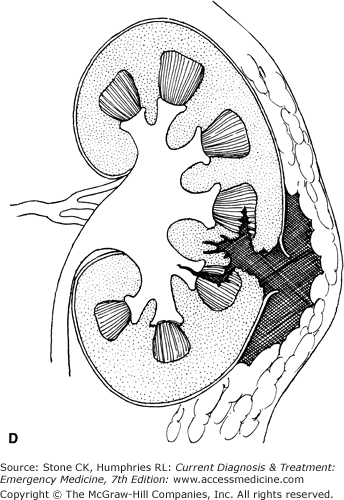
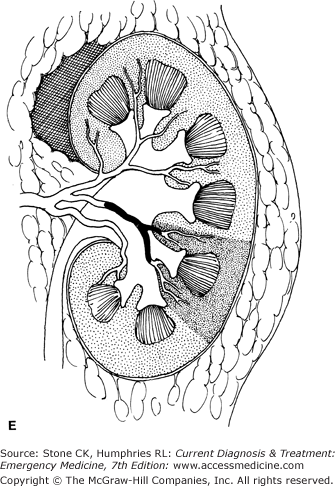
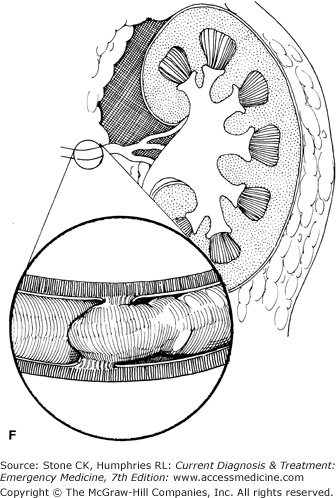
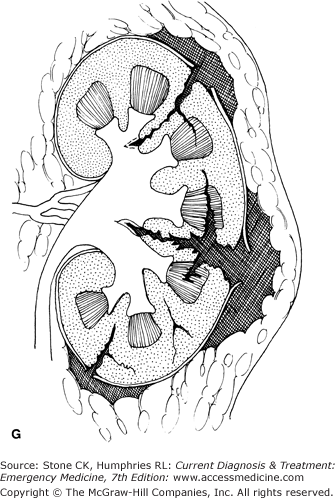
The diagnosis of renal trauma is complicated by the frequent presence of other peritoneal injuries, as well as the absence of any accurate markers for renal injury. Hematuria may be absent with significant renal injury (especially complete ureteropelvic avulsion), and the degree of hematuria does not correlate with the degree of injury when present. Renal injuries are graded on a scale of 1 to 5 (Figure 26–4). Following a general trend for the nonoperative management of many solid organ intra-abdominal injuries, 95% of renal injuries are managed without surgical exploration. However, only a special subset of patients with high-grade renal injuries are candidates for observation without surgical repair or nephrectomy.