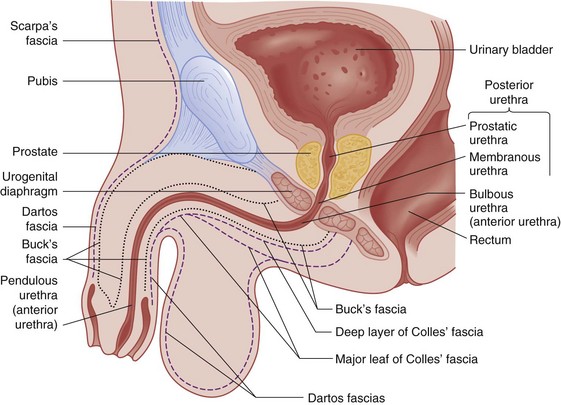
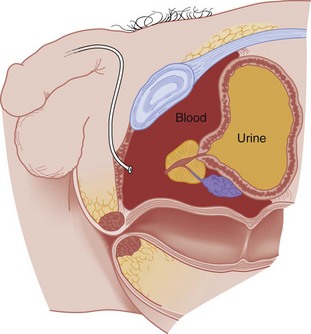
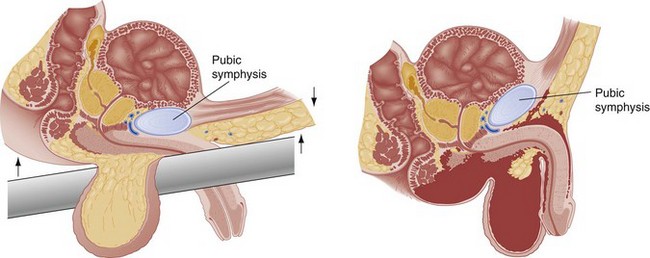
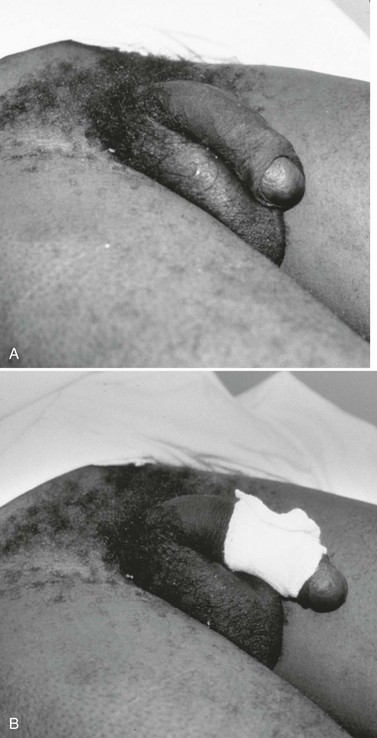
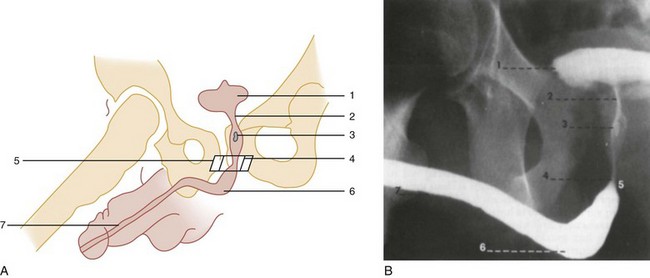
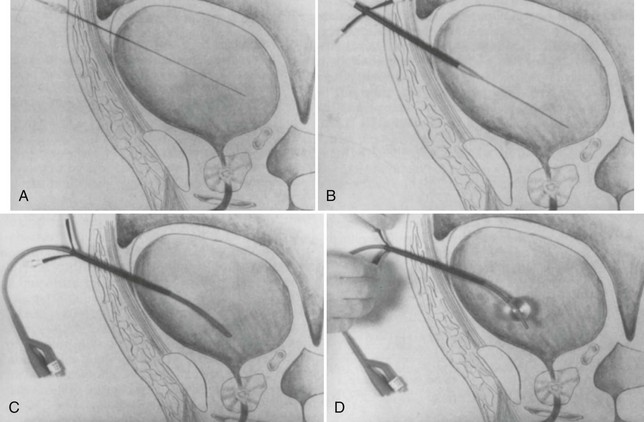
Chapter 47 Genitourinary trauma is frequently a covert entity and is associated with a wide array of injury. Approximately 10% of all multiply injured patients have some manifestation of genitourinary involvement.1 Because of its relatively infrequent occurrence and often subtle presentation, it may be overlooked in the initial evaluation of the multiply injured patient. Prompt identification and appropriate management of genitourinary injuries can minimize potential long-term complications, including renal insufficiency, chronic hypertension, incontinence, and sexual dysfunction. The astute emergency physician can accomplish these goals by a stepwise evaluation that considers the mechanism of injury, pertinent physical examination findings, urinalysis, and adjunctive diagnostic imaging. The basic tenets of lower urinary tract injury have not changed appreciably in recent decades. A thoroughly performed physical examination, pelvic radiography, and the recognition of gross hematuria or blood at the urethral meatus identify virtually all significant lower urinary tract injuries. Major advances in the identification of significant upper tract genitourinary injuries, their clinical markers, and ultimate staging procedures have come to the forefront over the last few decades. Before 1985, all trauma patients with any amount of microhematuria were labeled “at risk” for genitourinary injury and underwent intravenous pyelography. This was neither diagnostically definitive nor cost-effective and simply perpetuated the existing confusion and controversy. In 1985, Nicolaisen and colleagues published the first of a series of articles that established guidelines for identifying significant upper tract genitourinary injuries, their markers, and the diagnostic studies that define the exact extent of these injuries and aid in subsequent patient management.2 In addition, the advent of ultrasonography has greatly simplified the diagnosis and management of external genitalia trauma. Examination of the genitalia can be informative. The emergency physician should examine for evidence of hematoma or ecchymosis of the penile shaft, scrotal skin, or perineum. Gross blood at the urethral meatus is suggestive of a urethral injury and suggests the need for retrograde urethrography. In circumstances in which emergency surgical exploration for life-threatening injuries is indicated, retrograde urethrography can be performed in the operating room or after the operative procedure. For the male patient, classic teaching dictates that a Foley catheter should never be introduced when urethral injury is possible without prior evaluation of urethral integrity by retrograde urethrography. The concern is that trauma from the catheter placement may convert a partial urethral tear into a complete disruption. Although the literature on this topic is sorely lacking, one small retrospective review of 13 cases of urethral injury demonstrated no evidence that a careful blind attempt to insert a urinary catheter worsened the initial injury.3 Careful inspection for blood at the vaginal introitus is particularly important in the female patient known to have a pelvic fracture. A vaginal examination can discern vaginal lacerations or urethral disruption caused by displaced bony pelvic fracture fragments. This examination should be conducted carefully so as to protect the hands of the examiner from injury as well as to prevent worsening of the injuries themselves. Urethral injuries are uncommon in female patients owing to the short length and increased mobility of the female urethra and the relative protection from injury afforded by the symphysis pubis. Unlike with male urethral injuries, urethrography is technically difficult and not routinely recommended in females with suspected urethral injury. The inability to pass a Foley catheter in a premenopausal female patient with a pelvic fracture signifies the potential for urethral injury and possible need for suprapubic urinary drainage. Successful passage of a Foley catheter in a patient with blood at the vaginal introitus does not exclude urethral injury, however, and these worrisome physical examination findings are conveyed to the urologist, who can plan subsequent endoscopic or radiographic urethral evaluation accordingly.4–6 In an older postmenopausal female trauma patient, urethral injury is distinguished from a superiorly retracted urethral meatus and accompanying meatal stenosis. These preexisting conditions are common in an atrophic vaginal setting, and a 12- or 14-Fr coudé or Foley catheter usually is required to achieve successful bladder access. The digital rectal examination evaluates sphincter tone, bowel wall integrity, the presence or absence of gross blood, and the position of the prostate. Normally the posterior lobe of the prostate is palpable and well defined (Fig. 47-1). A pelvic fracture may disrupt the puboprostatic ligaments and the prostatomembranous urethra, resulting in significant retropubic venous bleeding. This may produce a large pelvic hematoma that can displace the prostate superiorly, resulting in a boggy, ill-defined mass on rectal examination (Fig. 47-2). Although it has long been recommended as part of the routine evaluation of all trauma patients, multiple studies have questioned the utility of the rectal examination in this setting and have specifically demonstrated that a palpably abnormal prostate is an insensitive indicator of urethral injury.7–10 Thus the decision to evaluate for urethral injury should consider additional clinical features, especially the presence or absence of gross hematuria or blood at the urethral meatus, and not rely on the findings of the rectal examination. The urogenital diaphragm divides the anterior (bulbous and pendulous) urethra from the posterior (membranous and prostatic) urethra. Contrary to early descriptions, the urogenital diaphragm does not completely encircle the membranous urethra, but rather forms an incomplete sling that offers posterior and lateral support.5 The prostatic urethra is attached to the posterior symphysis pubis by the puboprostatic ligaments. A fracture of the pelvis with displacement of the symphysis may result in a laceration or avulsion of the prostatic urethra because of the shearing force on the fixed prostatic and membranous urethra. Injuries to the anterior and posterior urethra are caused by different mechanisms, involve different symptoms, and are treated differently. Urethral disruption is the most significant injury to be identified. Failure to do so may lead to significant morbidity. Overly aggressive urethral manipulation can convert a partial urethral tear into a complete tear, thus precluding accurate assessment of urinary output and subsequently potentiating the long-term complications of urethral trauma (e.g., urethral stricture formation and urinary incontinence). Anterior urethral injuries are most often caused by straddle injuries, falls, gunshot wounds, and self-instrumentation (Fig. 47-3). Pelvic fractures account for most posterior urethral injuries (see Fig. 47-2). The risk of urethral injury varies with the specific type of pelvic fracture. High-risk fractures include the straddle fracture, in which all four pubic rami are involved, and the Malgaigne fracture, which involves fracture and displacement of the hemipelvis—that is, both ischiopubic rami anteriorly and the ipsilateral sacrum, sacroiliac joint, or ilium posteriorly. Urethral injuries are rarely associated with fractures that do not involve the ischiopubic rami.5,11 In a prospective, single-center study of 203 consecutive male patients with pelvic fractures, 51 sustained urethral injuries. Malgaigne and straddle fractures were significantly associated with urethral injuries, with odds ratios of 3.4 and 3.85, respectively. In the same series, the highest risk for urethral injury was seen in patients sustaining a straddle fracture with concurrent sacroiliac diastasis (odds ratio 24). Among those sustaining fractures not involving the anterior pelvic arch, none had urinary tract injury.11 Catheter Placement: The following technique for catheter placement assumes a normal urethra and includes the use of sterile technique, proper control of the foreskin, the use of copious amounts of lubricating jelly, and the gentle passage of a 14- or 16-Fr Foley or coudé catheter into the bladder. In all uncircumcised patients, continuous foreskin retraction with a folded 4 × 4-inch gauze pad is necessary to control the foreskin during catheter placement (Fig. 47-4). Without this maneuver, the foreskin tends to repeatedly reduce itself over the glans penis, which contaminates the field and complicates the catheterization attempt. Slight resistance to the advancing catheter should be expected secondary to voluntary contraction of the external sphincter. This is more apt to occur in a combative, anxious trauma patient than in a cooperative or unconscious patient. When this occurs, the patient should be reassured and asked to relax the perineum and rectal area while gentle advancing pressure is applied to the catheter. This combined approach allows the catheter to navigate the external sphincter successfully and pass easily into the bladder. If reassurance and relaxation do not allow easy passage of the catheter in a male patient with clinical features suggestive of urethral injury, it should be removed and retrograde urethrography performed. The catheter is passed to its fullest extent to ensure that the balloon is completely in the bladder when inflated, The catheter is then withdrawn to the point of balloon approximation with the bladder neck, secured to the patient’s leg to prevent accidental dislodgement, and left to drain. Inflation of the catheter balloon under any other circumstances may result in iatrogenic urethral trauma. Successful passage of a Foley catheter precludes a complete urethral disruption. Nonetheless, the possibility of a partial urethral injury not manifested by history, mechanism of injury, or physical examination does exist. If a possible urethral injury is suggested by physical examination findings before the placement of a Foley catheter, a retrograde urethrogram should be obtained. The presence of urethral extravasation together with contrast material filling the bladder is diagnostic of a partial urethral injury (Fig. 47-5). Identification of a partial urethral injury enables one careful attempt at urethral placement of a 12- or 14-Fr Foley or coudé catheter, depending on the size of the patient.6 If any difficulty is encountered, the catheter should be removed and a urologist consulted. If a partial urethral tear is suggested subsequent to successful passage of a Foley catheter, a small feeding tube can be placed alongside the urethral catheter and a modified retrograde urethrogram obtained. In this circumstance the urethrogram is for documentation and subsequent management purposes only because appropriate therapy (Foley catheter drainage) has already been instituted. Radiology: In male patients with possible urethral injury, retrograde urethrography is the diagnostic procedure of choice. Retrograde urethrography is not an emergency procedure and should follow more critical diagnostic and resuscitative measures. A preinjection kidney, ureter, and bladder (KUB) film is first obtained. In uncircumcised patients, the penile foreskin is retracted and secured with a folded 4 × 4-inch gauze pad (see Fig. 47-4). The penis should be held between the long and ring fingers of the nondominant hand. A simple Christmas tree adapter, a Cooke adapter placed on the end of a 60-mL Toomey syringe, or a Toomey syringe alone is gently passed into the urethral meatus until a snug fit inside the meatus is confirmed. The distal end of the syringe is secured with the thumb and index fingers of the nondominant hand (Fig. 47-6). Some authors have recommended inflation of a Foley catheter balloon just proximal to the fossa navicularis or the use of other cumbersome adjuncts to facilitate injection of contrast media. These techniques should be avoided, however, because they promote leakage of contrast material around the penis, which can simulate extravasation on the urethrogram and promote a spurious examination. Next, 60 mL (or 0.6 mL/kg in children) of full-strength or half-strength water-soluble contrast medium is injected slowly over 30 to 60 seconds. Overly forceful injection may result in intravasation of contrast material into the urethral venous plexus. A radiograph is taken during the injection of the last 10 mL of contrast material. Retrograde flow through the urethra and into the bladder without extravasation ensures continuity of the urethra and absence of urethral injury (Fig. 47-7). Extravasation of contrast material outside the urethra with concomitant evidence of bladder filling distinguishes a partial urethral injury (see Fig. 47-5) from a complete urethral disruption, in which contrast material will be absent from inside the bladder (Fig. 47-8). The latter situation requires urologic consultation for appropriate management, the timing and specifics of which remain controversial and depend on the location and mechanism of injury.6,12,13 In the interim, if measurement of urinary output is essential, the bladder should be accessed by the suprapubic placement of a peel-away sheath and Foley catheter through use of the Seldinger technique (Fig. 47-9). When venous intravasation of contrast is suggested, a postvoid film demonstrates clearing of any intravasated material while extravasated contrast from a urethral injury remains. Retrograde urethrography should be deferred if pelvic angiography is indicated, as extravasated contrast material from a urethral injury may obscure computed tomography (CT) scans and angiographic images and complicate attempts to control significant pelvic hemorrhage by vascular embolization.14 The optimal definitive management of urethral injuries remains a subject of controversy in the urologic literature.6,12,13 Pertinent variables include the location of the injury (anterior vs. posterior), extent of the disruption (partial vs. complete), mechanism of injury, hemodynamic stability of the patient, and presence of associated injuries. Treatment options vary from allowing a partial disruption to heal over a stenting urethral catheter to early or delayed, open or endoscopic repair. Adjunctive suprapubic urinary drainage is frequently indicated. Regardless of the specific management plan, the ultimate goals are the preservation of urinary continence and sexual function and avoidance of the disruption of any pelvic hematoma. In female patients, proximal urethral injuries are managed by immediate surgical exploration and repair, as conservative management with proximal urinary diversion alone is associated with an increased risk of urethrovaginal fistulae or obliterative urethral strictures. Distal injuries may be managed by urethral catheterization. Regardless of the location of the urethral injury, associated vaginal lacerations require transvaginal repair to reduce the incidence of fistula formation.6 More than two thirds of bladder injuries result from blunt trauma. Approximately 90% result from motor vehicle collisions (MVCs) as a result of trauma sustained during ejection from the vehicle or the compressive force of the seat belt on a distended bladder. Approximately 80% of blunt bladder injuries are associated with fractures of the bony pelvis.15 Additional life-threatening, nonurologic injuries are common and confer a significant mortality risk.15,16 Penetrating injuries may be inflicted by gunshot wounds, stab wounds, or impalement injuries. The diagnostic evaluation of the bladder, like that of the urethra, can be accomplished quickly without elaborate radiographic equipment or can be part of the CT evaluation performed for the evaluation of nonurologic injuries. Extraperitoneal rupture occurs almost exclusively with pelvic fractures when the associated shearing forces result in tearing of the anterolateral bladder wall at its fascial attachments. Occasionally, extraperitoneal rupture results from bladder laceration by a bone spicule from the fractured pelvis.15 Extravasated urine may be confined to the perivesical space or may dissect along tissue planes and extend to the penis, scrotum, thigh, anterior abdominal wall, obturator foramen, or retroperitoneum.15,17,18
Genitourinary System
Perspective
Historical Perspective
Clinical Features
Physical Examination
Lower Urinary Tract
Anatomy
Pathophysiology
Diagnostic Strategies
Management
Bladder Trauma
Pathophysiology

Full access? Get Clinical Tree


Genitourinary System



Only gold members can continue reading. Log In or Register to continue




