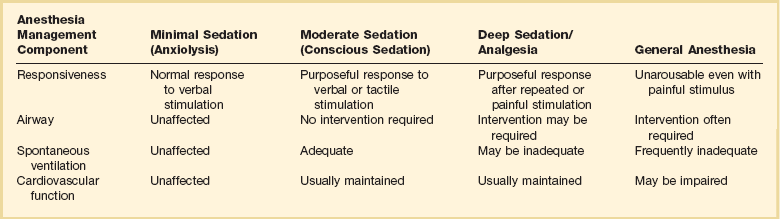
17 The first documented endoscopic foray into the human body was performed by Philip Bozinni in the early 1800s, when he used a speculum fitted with a candle and mirror to examine the urinary tract.1 The first gastroscopy was performed in 1868 by German physician Adolf Kussmaul, with a rigid metal tube passed carefully down a patient’s esophagus into his stomach. In 1932, Rudolph Schindler, in collaboration with a German engineer, Georg Wolff, developed a semiflexible instrument with a flexible distal shaft. Although this device was hailed as the first safe workable gastroscope, it was not without limitation, including incomplete visualization of the esophagus and stomach, patient discomfort, and absence of photographic documentation.2 Fiberoptics were introduced into the endoscope in 1957 by Basil Hirschowitz, and in the 1960s and 1970s further advancements were made with endoscope length, improved visualization, and greater control. Video cameras and monitors were subsequently incorporated into endoscopic technology, allowing others to view what was previously available only to the endoscopist. Early experience with rigid and semiflexible proctosigmoidoscopes and colonoscopes was disappointing because of the tortuous nature of the sigmoid and colon, and early fiberoptic instruments fared no better. Bergein Overholt made adjustments in torque and control to develop a prototype flexible fiberoptic instrument in 1963.3 The first total colonoscopy was performed in Sardinia, Italy, in 1965. Luciano Provenzale and Antonio Revignas instructed a patient to swallow a piece of polyvinyl tubing, which ultimately emerged from the anus. They attached a side-viewing gastroscope and gently pulled it through the entire colon to the cecum.3 Further refinements were carried out in England, the United States, and Japan, and in 1969 Hiromi Shinya performed the first polypectomy, removing a 1.5 cm pedunculated polyp from the sigmoid colon of a 70-year-old Chinese gentleman.4 Shortly thereafter, colonoscopy became a routine procedure performed by gastroenterologists and other health care providers all over the world. Endoscopic cannulation of the duodenal ampulla was first accomplished in Chicago by William S. McCune and colleagues in 1968 and is considered the first reported case of endoscopic retrograde cholangiopancreatography (ERCP).5 Sphincterotomy was performed in 1974 facilitating removal of two common bile duct stones6 and ushering in a new era of therapeutic pancreaticobiliary endoscopy. Today, ERCP remains an invaluable procedure in evaluating and treating diseases of the pancreas and biliary tract. The first ultrasound examination within the gastrointestinal (GI) lumen was performed by physician John Julian Wild and electrical engineer John Reid in 1956, when they developed the transrectal ultrasound probe.7 The incorporation of ultrasound into a standard endoscope occurred in 1976, when Lutz and Rosch passed an ultrasound probe through an accessory port of an endoscope. Further improvements were achieved by Strohm and colleagues and Eugene DiMagno and coworkers, who introduced their own prototype echoendoscopes in 1980. The first endoscopic ultrasound (EUS)–guided fine-needle aspiration was performed on submucosal lesions of the stomach in 1991 by Giancarlo Caletti.8 EUS equipment differs from the standard endoscope in that an ultrasound transducer is incorporated into the distal end of the insertion tube. The transducer emits sound waves that are directed at adjacent tissues and deflected back to the transducer. Individual tissues have different acoustic qualities. Radial and linear echoendoscopes are currently available. Interventional procedures, such as fine-needle aspiration and injections, may be performed safely with the latter echoendoscope.9 All video endoscopes have an image sensor called a charge-coupled device (CCD) mounted at the tip of the endoscope, which transmits an image to a video processor for display. Advances in CCD technology have resulted in the current high-resolution or high-definition (HD) endoscopes, which produce signal image resolutions that range from 850,000 pixels to more than 1 million pixels, allowing for detailed inspection of the GI mucosa.10 The wireless video capsule is a small disposable unit containing a small camera, short focal length lens, light source, two batteries, and a radio telemetry transmitter.11 There are presently three types of video capsules: an esophagus-specific capsule incorporating two CCD chips oriented at 180 degrees, a small bowel video capsule employing a single CCD chip with an 8-hour battery capacity, and experimental colonic video capsules utilizing time-sensitive deactivation and reactivation of the illumination and telemetry elements in order to preserve battery power during small bowel transit. Accessory devices have allowed endoscopic advancement of activated video capsules into the small intestine of patients who have dysfunctional esophageal and gastric motility or altered upper GI anatomy due to prior surgery. The capsule is activated by removal from a magnetic holder, and battery life is approximately 8 hours. Two frames per second are captured by the camera and transmitted to a data recorder that is carried by the patient. Data are downloaded from the recorder to a personal computer and interpreted. Handheld devices have also recently been developed to allow real-time monitoring of video capsule images. Choice of anesthesia is based on patient profile, the endoscopic procedure, and preference of the endoscopist, anesthesiologist, and patient. Essential patient information includes prior adverse events from anesthesia, current medications, pertinent medical history, cardiopulmonary status, age, allergies, body habitus, and social history. Patients with alcohol or narcotic dependency may require high doses of opiates and benzodiazepines. Agents such as propofol may facilitate their sedation. Pregnancy should be excluded in any woman of childbearing age. The level of sedation also depends on the endoscopic procedure. Flexible sigmoidoscopy and esophagogastroduodenoscopy (EGD) may require minimal or moderate sedation, whereas more complex and lengthier procedures, such as ERCP and EUS, may require deep sedation or even general anesthesia. Table 17.1 illustrates the different depths of sedation as defined by The American Society of Anesthesiologists Task Force.12 Table 17.1 Levels of Sedation and Anesthesia Adapted from Gross JB, Bailey PL, Connis RT, et al. Practice guidelines for sedation and analgesia by non-anesthesiologists. Anesthesiology 2002;96:1004-1017. Regardless of the type of sedation, cardiopulmonary status should be monitored at all times. Standard equipment should include a pulse oximeter, continuous electrocardiogram, and cyclical blood pressure monitoring. Personnel trained in airway support should always be present. The cardiopulmonary complication rate is 0.005% for EGD and 0.01% for colonoscopy.13 Four drug types are commonly used in GI endoscopies: pharyngeal anesthesia, benzodiazepines, opiates, and propofol. Pharyngeal anesthetics, such as lidocaine, benzocaine, and tetracaine, are used to suppress the gag reflex during upper GI tract procedures. These agents, applied by spray or gargling, are active for approximately 1 hour. Potential risks include aspiration owing to loss of gag reflex and, rarely, methemoglobinemia.14 Benzodiazepines, such as midazolam and diazepam, are used to induce relaxation and amnesia by binding to receptors of the postsynaptic γ-aminobutyric acid neurons. Both have similar properties, with the latter possessing a longer half-life and milder amnestic properties.15 Onset of action occurs in 1 to 2.5 minutes with intravenous midazolam and 8 minutes with diazepam.16 Adverse reactions include respiratory depression and hypotension. Overdoses can be reversed with flumazenil, although caution should be used because seizures secondary to acute withdrawal may occur. Opiates such as fentanyl and meperidine are used for analgesia and sedation. A synergistic effect occurs when opiates are given concurrently with intravenous benzodiazepines. Fentanyl has a rapid onset (1.5 minutes) with a short duration of action (0.5 to 1 hour), whereas meperidine has an onset of 5 minutes and lasts 3 to 5 hours.16 Common adverse reactions include respiratory depression, hypotension, constipation, nausea, and vomiting. Overdosage can be reversed with naloxone, an opioid antagonist. Long-term opiate users may experience acute withdrawal symptoms with naloxone. Serotonin syndrome may occur if monoamine oxidase inhibitors are used with meperidine. Propofol, an ultra-short-acting anesthetic agent, has been increasingly used in recent years.17 Propofol has a rapid onset of action, deeper levels of sedation, and faster recovery time compared with narcotics and benzodiazepines.18 Propofol use during colonoscopy has been shown to carry a lower risk of cardiopulmonary complications compared with traditional agents.19 Controversies exist as to its cost-effectiveness and the requirement that it be administered exclusively by an anesthesiologist. EGD is one of the most commonly performed procedures in the world and has become the primary tool for evaluating the esophagus, stomach, and proximal portion of the duodenum. EGD is performed for a wide variety of indications and has a diagnostic and therapeutic role (Box 17.1). There are relatively few contraindications to upper endoscopy (Box 17.2). EGD is a safe procedure. Perforation occurs in approximately 0.05% to 0.70% of patients,20 with the higher incidence in patients undergoing therapeutic intervention (i.e., biopsy, dilation, mucosal resection). Bleeding may occur as a result of Mallory-Weiss tears, cautery injury, or sclerotherapy injection and after biopsy or polypectomy. Prior to undergoing elective EGD, patients should be fasting for at least 6 hours. Motility agents, such as erythromycin, may be beneficial in clearing the stomach of blood or food.21 In situations of possible airway compromise, elective intubation is reasonable. A 20% incidence of aspiration pneumonia was initially demonstrated after emergent EGD for upper GI bleed.22 A subsequent retrospective study of 220 patients failed to show any significant difference in post-EGD pulmonary infiltrates, witnessed aspiration, cardiopulmonary complications, or in-hospital mortality rate.23 Despite the lack of a conclusive double-blinded randomized trial, endotracheal intubation may be appropriate in patients with active hematemesis, altered mental status, unstable cardiopulmonary function, or agitation. Alternatives to intubation may include pre-endoscopy lavage, overtube placement, or the use of large-caliber endoscopes for suction. Thermal cautery probes deliver predetermined pulses of heat (250° C) to an endoscopic catheter tip, which is transferred to tissue on contact.24 Thermal probe coagulation can be applied to peptic ulcers, vascular lesions, and Mallory-Weiss tears. Another option for contact thermal coagulation is monopolar or bipolar electrocautery. With electrocautery, electrical current flows from electrode tip through contacted tissue. Monopolar cautery requires attaching an electrical ground to the patient and may cause extensive burn injuries and tissue stickiness. Monopolar cautery is typically not used for hemostasis, but serves a role in snare polypectomy. Bipolar cautery consists of two active electrodes incorporated into a single catheter probe, allowing electrical current to pass from one electrode through the tissue and back to the other electrode. Consequently, bipolar cauterization allows for improved control of coagulation depth. Injection therapy for nonvariceal and variceal bleeding is performed with sclerotherapy injector needles. Solutions commonly employed are epinephrine in saline (1 : 10,000) and sclerosing agents, such as polidocanol and ethanolamine. Epinephrine reduces bleeding by vasoconstriction, vessel tamponade, and platelet aggregation.25,26 The potential exists for systemic side effects from submucosal injections because plasma epinephrine levels can transiently increase four to five times above basal levels.27 To date, only a single case of hypertension and ventricular tachycardia after epinephrine injection has been reported.28 Sclerosing agents achieve hemostasis through inflammation and sclerosis and have been employed in peptic ulcer hemorrhage and variceal bleeding. Mediastinitis, perforation, stricture formation, and infection are among the reported complications.29 Injector needles are also used in nonbleeding situations. Polyps and superficial tumors can be raised with submucosal injection of saline or epinephrine prior to polypectomy. This technique reduces the likelihood of postpolypectomy hemorrhage or perforation.30 Lesions requiring surgery can be tattooed with ink to facilitate localization by the surgeon. Rubber band ligation is an effective tool for hemostasis. The delivery system is loaded onto the endoscope tip, and current models allow for deployment of multiple rubber bands before reloading. For variceal bleeding, endoscopic variceal ligation has become the treatment of choice and is superior to endoscopic sclerotherapy in speed of variceal eradication, decreased risk of recurrent bleeding, and fewer complications.31 Other uses of banding include gastric varices, peptic ulcers, Dieulafoy’s lesions, postpolypectomy hemorrhage, and internal hemorrhoids. Metal clips, or endoclips, have been used successfully for GI bleeding,32 closure of perforations,33 anastomotic leaks,34 and prevention of postpolypectomy bleeding.35 The potential for significant tissue injury is small as only the mucosal and submucosal layers are involved in the grasping.36 The procedure may be technically challenging if massive bleeding is present, or the angle of approach is tangential to the lesion.37 Laser therapy, utilizing neodymium:yttrium-aluminum-garnet (Nd:YAG) or argon, is delivered through probes passed via the endoscope to treat bleeding lesions and for tumor ablation. Nd:YAG and argon lasers differ in the width and depth of tissue effect, with the former having the greater effect.38 Advantages of laser therapy include improved accuracy and not requiring direct contact with the desired target. Argon plasma coagulation is a noncontact method of hemostasis that delivers argon gas through a catheter probe. The argon gas is ionized, delivering thermal energy to adjacent target tissue. Large areas and tissue not in direct view, due to the tangential arcing nature of the argon gas, can be treated rapidly. Clinical uses include adjunctive ablative therapy after piecemeal resection of colonic polyps, radiation proctopathy, GI vascular lesions, bleeding peptic ulcers, Barrett’s esophagus ablation, and palliation of GI malignancies.39,40 Tissue adhesives constitute a newer class of agents for GI hemostasis. The major types of tissue adhesives are fibrin sealants and cyanoacrylate. Fibrin sealants form a coagulum through the interaction of fibrinogen, factor XIII, and thrombin.41 Extensively used in the surgical fields for tissue adhesion, hemostasis, and wound care, fibrin sealants also have been used endoscopically in bleeding peptic ulcers,42 variceal bleeding,43 and GI fistulas.44 Cyanoacrylate is synthetic glue that rapidly polymerizes into a solid complex when in contact with water or blood.45 Cyanoacrylate has been used with success for esophageal and gastric varices.46,47 A serious complication of tissue adhesives is embolization and infarction.48 In addition to hemostasis, upper endoscopy is routinely employed for other therapeutic situations. Foreign object ingestion and food bolus impaction occur commonly. Although most foreign bodies pass spontaneously, up to 20% of cases may require endoscopic intervention. Various types of endoscopy, ranging from rigid to flexible, and equipment (Box 17.3) are available for foreign body retrieval. An overtube is available for airway protection and frequent esophageal intubations. Retrieval should be performed within 24 hours or more urgently if the ingested object is sharp, is a disc battery, or is causing the patient pain or difficulty in handling secretions. If it is not possible to remove the object endoscopically and it is less than 2.5 cm, the object can be gently maneuvered into the stomach, from which spontaneous passage usually occurs.49 Unsuccessful removal or obstruction requires surgical evaluation. Esophageal narrowing is a common reason for recurrent food impaction. Narrowing may occur from benign conditions, such as peptic strictures and Schatzki’s rings, or malignancy compressing the lumen. Endoscopic dilation can be performed on anatomic narrowings of the esophagus, pylorus, and anastomotic strictures. Four types of dilators are currently available: tip-weighted push bougies (Maloney or Hurst), wire-guided dilators (Savary-Gilliard or American), through-the-scope dilating balloons, and clear optical dilators that allow direct endoscopic visualization. Dilation also is indicated in patients with achalasia, although recurrence is common, and clinical efficacy is decreased with subsequent dilations.50 In general, endoscopic dilation increases the risk of perforation, with reported rates between 0.1% and 0.4%.51
Gastrointestinal Endoscopy
History
Endoscopic Equipment
Anesthesia
Esophagogastroduodenoscopy

Full access? Get Clinical Tree


Anesthesia Key
Fastest Anesthesia & Intensive Care & Emergency Medicine Insight Engine






