Diarrhea and Vomiting
Diarrhea and vomiting are common reasons for Emergency Department visits. Although the majority of cases are of an infectious, self-limiting nature, the differential diagnosis is broad with the potential for significant morbidity and mortality. Many pathologic processes involve gastrointestinal (GI) symptoms. Included are intracranial pathology (trauma, masses, infections), cardiac disease (myocardial infarction, angina), toxic exposures (digoxin, carbon monoxide, heavy metals), acute abdominal pathology (intestinal obstruction, mesenteric ischemia), and endocrine abnormalities (diabetic ketoacidosis, adrenal insufficiency), among others. In addition, infectious causes of diarrhea and vomiting can cause significant harm, especially in the elderly, in infants, and in immunocompromised individuals (Figure 36–1).
Immediate Management of Life-Threatening Problems
- Signs of decreased perfusion
- Hypotension, tachycardia, oliguria, and orthostasis
- Cool, pale skin; dry mucous membranes; and altered mentation
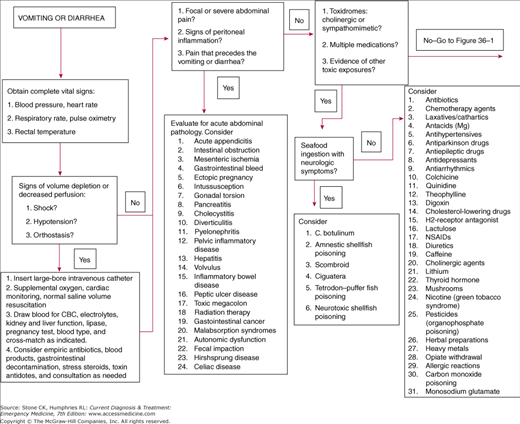
Obtain complete vital signs. Look for signs of decreased perfusion (ie, cool, pale skin; altered mentation; decreased urinary output; dry mucous membranes). Hypotension (systolic pressure <90 mm Hg), tachycardia, oliguria, and orthostasis may indicate impending hemodynamic instability. Look for evidence of sepsis, GI bleed, cardiac pump dysfunction, surgical abdominal pathology, toxic exposures, endocrine abnormalities, or anaphylaxis.
Insert a large-bore intravenous catheter and draw blood for a complete blood count (CBC), electrolytes, renal and liver function, serum lipase, and a pregnancy test, if indicated. Type and crossmatch if significant blood loss is reported or suspected. Start supplemental oxygen, cardiac monitoring, and pulse oximetry together with normal saline volume resuscitation while the underlying cause is sought. If appropriate, initiate empiric antibiotic therapy. Hospitalize the patient for continuous monitoring, supportive treatment, and further investigation if the cause is uncertain. Initiate specific treatment once the cause is determined.
- Focal abdominal pain or signs of peritoneal inflammation (rebound)
- Pain that precedes the vomiting or diarrhea
- Pain out of proportion to the physical examination
Patients with acute surgical abdominal pathology may present with diarrhea and vomiting and are at risk of being mislabeled as having gastroenteritis. Inquire about the nature and location of pain and the existence of upper GI symptoms (vomiting) and lower GI symptoms (diarrhea). Determine which symptom began first. Signs and symptoms suggestive of an acute abdominal emergency include focal abdominal pain, an examination consistent with peritoneal inflammation, pain that precedes the vomiting and diarrhea, protracted vomiting with nonspecific abdominal pain, and pain out of proportion to the physical examination. Consider entities such as acute appendicitis, intestinal obstruction, mesenteric ischemia, ectopic pregnancy, GI bleed, intussusception, and gonadal torsion (Table 36–4). Serial abdominal examinations in the ED may help differentiate early acute abdominal emergencies with vomiting or diarrhea from gastroenteritis. In patients with arteriovascular disease who present with pain out of proportion to the examination, mesenteric ischemia must be ruled out.
Treatment ultimately depends on the cause of the symptoms. Obtain complete vital signs; gain intravenous access; and draw blood for a CBC, electrolytes, renal and liver function tests, serum lipase, pregnancy test if appropriate, and blood type and crossmatch. An acute abdominal series may demonstrate a small or large bowel obstruction. A computed tomography (CT) scan or ultrasound may help identify the cause of the acute abdomen. If intussusception is suspected, an air contrast or barium enema can be both diagnostic and therapeutic. If the patient’s condition is unstable, seek appropriate surgical consultation early.
- Cholinergic or sympathomimetic syndromes
- Ingestion of mushrooms, herbal or plant preparations, or seafood
- Occupational exposures—exposure to heavy metals, pesticides, or carbon monoxide
- Medications—digoxin, salicylates, or others
Diarrhea and vomiting are often the presenting symptoms of toxic exposures. The list of toxins is extensive (Figure 36–1). Obtain key historical information including medications, occupational exposures, use of herbal preparations, consumption of mushrooms or plant products, ingestion of seafood, exposures to heavy metals, and a history of allergic reactions. Search for specific toxin-induced syndromes such as cholinergic or sympathomimetic reactions. Consider common toxins such as digoxin, salicylates, and carbon monoxide. If neurologic symptoms exist, consider botulism or shellfish poisoning.
Begin treatment with the proper decontamination method. Give patients with toxic ingestions activated charcoal and a cathartic. Patients with cutaneous and inhalation exposures should be removed from the source and the contaminant diluted. Initiate supportive care and continuous monitoring. Administer specific antidotes if appropriate.
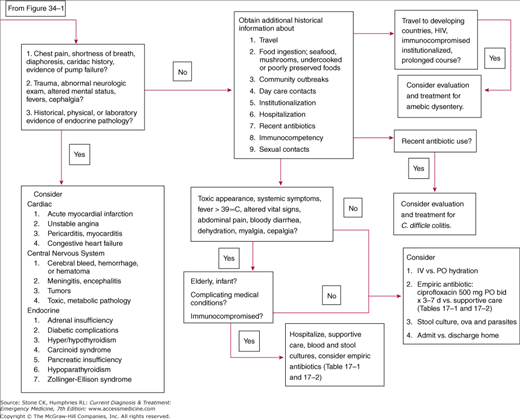
- Chest pain, shortness of breath, diaphoresis, acute pump failure
- History of cardiac, central nervous system, endocrine disease, or trauma
- Abnormal neurological examination, alteredmentation, fevers, headache
- Laboratory and physical abnormalities
Cardiac, central nervous system, or endocrine disorders may include vomiting or diarrhea as presenting symptoms (Figure 36–1). Evidence of a cardiac-related disorder includes chest pain, shortness of breath, diaphoresis, a history of cardiac disease, or evidence of acute pump failure. Indications of central nervous system pathology include a history of trauma, an abnormal neurological examination, fever, headache, and evidence of other toxic or metabolic pathology affecting the central nervous system.
Patients with a suspected cardiac, central nervous system, or endocrine causes of vomiting or diarrhea should receive aggressive evaluation and management. This may include an ECG, continuous cardiac monitoring, intravenous access, supplemental oxygen, pulse oximetry, and a complete set of labs including clotting studies and cardiac enzymes as indicated. Obtain X-rays, CT scans, and consultations as needed.
Further Evaluation of the Patient with Diarrhea and Vomiting
Once life-threatening conditions have been sought and treatment begun, an attempt should be made to further identify the cause of vomiting and diarrhea. Consider the following historical, physical, and laboratory investigations (Table 36–1).
History
Physical examination
Laboratory and diagnostic studies
|
Important features of the present illness include time of onset, the nature of symptoms, and duration of illness. Differentiate acute (less than 2 weeks) from chronic symptoms. Clarify the patient’s use of the term diarrhea. Identify associated symptoms. Inquire about fever, abdominal pain, anorexia, diarrhea, constipation, tenesmus, myalgias, vomiting, cephalgia, and neurologic symptoms such as paresthesias, weakness, or cranial nerve palsies. Inquire about the presence of blood or mucus in the stool and about the character of the vomitus (bloody or bilious). Determine the onset and severity of diarrhea and vomiting in relation to other symptoms. Abdominal cramps after copious, watery diarrhea is consistent with gastroenteritis. However, abdominal pain followed by nausea and loose stool could represent appendicitis. The symptom complex of profuse diarrhea, fever, myalgias, and cephalgia is consistent with dysentery, whereas a symptom complex of sudden severe headache, nausea, vomiting, and loose stool could represent a process such as subarachnoid hemorrhage.
Inquire about the patient’s medical and surgical history. Give special attention to immunocompetency. Inquire about a history of HIV, diabetes mellitus, GI bleed, abdominal surgeries, malignancies, and endocrine disease. Ask about recent chemotherapy or radiation therapy.
Inquire about medications including prescription, over-the-counter, herbal preparations, and drugs of abuse. Give particular attention to recent antibiotic or laxative use.
Ask about common source exposures such as daycare or community outbreaks. Inquire about a history of hospitalization or institutionalization.
Inquire about unusual foods, dairy products, eggs, seafood, or unpasteurized or undercooked food. Ask about the ingestion of mushrooms or other plant products.
Inquire about recent international travel, especially to developing countries. Forty percent of travelers to endemic regions of Latin America, Asia and Africa acquire traveler’s diarrhea. Ask about recent domestic travel or outdoor activities, especially backpacking or exposure to new water sources.
Assess the risk of exposure to toxins, including heavy metals, carbon monoxide, salicylates, and digoxin (see Figure 36–1). Ask about occupational history as it relates to toxin exposures. In farm workers, consider pesticides (organophosphate poisoning) and nicotine (green tobacco syndrome). Inquire about a history of allergic reactions.
Inquire about sexual contacts. Amebiasis, giardiasis, campylobacteriosis, salmonellosis, and shigellosis can be transmitted by sexual contact. Chlamydia trachomatis, herpes simplex, and Neisseria gonorrhoeae are also possible causes of lower GI symptoms. HIV-positive and immunocompromised individuals are subject to infections with Cryptosporidium, cytomegalovirus, and Mycobacterium avium intracellulare.
Use the physical examination to assess the patient’s hydration status, evaluate for sepsis, rule out the acute abdomen, and determine the presence of blood in the stool.
Assess the patient’s overall health. Look for evidence of volume depletion, a toxic appearance, or jaundice.
Fever is consistent with invasive bacterial or parasitic causes of gastroenteritis (ie, dysentery). Fever could also indicate a process requiring acute surgical intervention. Less commonly, fever may be associated with a viral or noninvasive bacterial gastroenteritis. Food poisoning should not be associated with fever.
Hypotension and tachycardia are typical responses to volume depletion. If the volume status is not apparent, evaluate for orthostasis with the patient supine, sitting, and standing to detect more subtle degrees of volume depletion (systolic pressure drop ≥10 mm Hg and pulse rise ≥15 beats/min). Young, healthy adults may maintain normal vital signs even with significant dehydration. Look for a blunted response in patients who are taking atrioventricular nodal blockers.
Significant abdominal pain should prompt the search for causes other than infectious gastroenteritis. If abdominal examination elicits focal tenderness, or if signs of peritoneal inflammation are present, consider acute surgical pathology. However, subjective, diffuse, and crampy abdominal pain or tenderness may occur after extensive vomiting or diarrhea. In addition, several infectious agents, most notably Yersinia enterocolitica and Campylobacter sp., may mimic appendicitis and cause right lower quadrant pain, anorexia, low-grade fever, and vomiting preceding the onset of diarrhea. Appendicitis must be ruled out in patients with this presentation.
Perform rectal examination to detect fecal impaction, melena, or hematochezia.
Laboratory and diagnostic tests are of limited value in the routine evaluation of diarrhea and vomiting. Testing should be carried out, as indicated, in patients with a suspected noninfectious cause of vomiting or diarrhea, in those who are hemodynamically unstable, the very young, the elderly, and immunosuppressed individuals. In addition, testing may be necessary in patients with a prolonged course or in those not responding to conservative management.
Fecal erythrocytes and, to a greater degree, leukocytes have been used as a guide to determine who should receive empiric antibiotics. Both findings are associated with inflammatory diarrhea, of which bacterial dysentery is a common cause. However, there are many noninfectious causes of inflammatory diarrhea, which may also produce fecal red and white cells. These include inflammatory bowel disease (IBD), chemotherapy and radiation therapy, hypersensitivity, and autoimmune disorders. Just as the presence of erythrocytes and leukocytes is not specific for a bacterial process, their absence by stool smear does not rule it out. Furthermore, the cell count has not been shown to be a good indicator of which patients will benefit from empiric antibiotic treatment.
Consider bacterial culture of stool in patients experiencing a prolonged course, in infants, in the elderly, in immunocompromised patients, and in patients who appear toxic. Stool for culture can be collected in the emergency department, and, in the event that the diarrhea persists, results can be used to guide future treatment.
Consider testing for ova and parasites in patients with chronic diarrhea, those with a history of travel to developing countries, patients with HIV infection, and those with exposure to infants in daycare.
Consider testing for C. difficile toxin if the patient reports recent antibiotic use or recent hospitalization. Diarrhea may be delayed as long as 12 weeks after antibiotic therapy. Clindamycin, penicillins, and cephalosporins are commonly implicated. The incidence of community-acquired infection without recent antibiotic use is well established. Consider testing in patients with severe diarrhea, abdominal pain, and foul-smelling stool, even in those without recent antibiotic use.
Test patients with suspected hemolytic-uremic syndrome for E. coli 0157:H7 toxin through a stool culture looking specifically for 0157:H7 or if available by identifying the toxin through rapid immunoassay.
Consider testing for Giardia antigen in HIV-infected patients, in those with a history of travel to developing countries or a history of backpacking, and in those with daycare exposure.
Order other blood tests as indicated, especially if significant dehydration is suspected. Liver function testing is helpful if biliary colic or cholecystitis is suspected as the cause of vomiting. Lipase should be ordered in the patient with a history of pancreatitis, significant alcohol use or epigastric pain.
A urinalysis and a urine pregnancy test should be obtained if indicated.







