![]() Unstable patients with gastroesophageal varices receiving maximal medical therapy
Unstable patients with gastroesophageal varices receiving maximal medical therapy
![]() Endoscopy is unavailable or unsuccessful
Endoscopy is unavailable or unsuccessful
CONTRAINDICATIONS
![]() Esophageal strictures or recent gastroesophageal surgery
Esophageal strictures or recent gastroesophageal surgery
![]() Relative:
Relative:
![]() No active bleeding
No active bleeding
![]() Incomplete equipment
Incomplete equipment
![]() Source of bleeding likely gastric
Source of bleeding likely gastric
![]() General Basic Steps
General Basic Steps
![]() Gather supplies
Gather supplies
![]() Prepare patient—intubate
Prepare patient—intubate
![]() Placement and gastric balloon inflation
Placement and gastric balloon inflation
![]() Traction
Traction
![]() Esophageal balloon inflation
Esophageal balloon inflation
SUPPLIES
![]() Sengstaken–Blakemore (SB) tube (triple lumen tube) or Minnesota tube (quadruple lumen tube). The fourth port is for suctioning the proximal esophagus.
Sengstaken–Blakemore (SB) tube (triple lumen tube) or Minnesota tube (quadruple lumen tube). The fourth port is for suctioning the proximal esophagus.
![]() Salem Sump (double-lumen nasogastric tube) and silk ties to create necessary fourth lumen (not needed if using a Minnesota tube)
Salem Sump (double-lumen nasogastric tube) and silk ties to create necessary fourth lumen (not needed if using a Minnesota tube)
![]() 60-mL Luer lock syringe
60-mL Luer lock syringe
![]() 60-mL Piston syringe
60-mL Piston syringe
![]() 2 Christmas tree catheter adapters
2 Christmas tree catheter adapters
![]() 2 Three-way stopcocks
2 Three-way stopcocks
![]() 2 Heplock caps
2 Heplock caps
![]() Surgilube
Surgilube
![]() 1 Sterile gauze bandage roll (Kerlix)
1 Sterile gauze bandage roll (Kerlix)
![]() 1 L NS (normal saline)
1 L NS (normal saline)
![]() Kelly clamps (padded)
Kelly clamps (padded)
![]() 2 wall-suction units
2 wall-suction units
![]() Straight connector
Straight connector
![]() Manual sphygmomanometer
Manual sphygmomanometer
TECHNIQUE
![]() Preparation
Preparation
![]() Secure the airway. The patient will be intubated in almost all scenarios. Raise the head of the bed to 45 degrees.
Secure the airway. The patient will be intubated in almost all scenarios. Raise the head of the bed to 45 degrees.
![]() Assemble attachments to gastric balloon and esophageal balloon ports
Assemble attachments to gastric balloon and esophageal balloon ports
![]() Test for air leaks using 60-cc Luer lock syringe
Test for air leaks using 60-cc Luer lock syringe
![]() Gastric balloon—Inflate 250-cc air
Gastric balloon—Inflate 250-cc air
![]() Esophageal balloon—Inflate 60-cc air
Esophageal balloon—Inflate 60-cc air
![]() Deflate the balloons completely
Deflate the balloons completely
![]() If using an SB tube, create fourth lumen:
If using an SB tube, create fourth lumen:
![]() Place the distal tip of Salem Sump 2 cm proximal to the esophageal balloon and secure with silk ties (FIGURE 29.1)
Place the distal tip of Salem Sump 2 cm proximal to the esophageal balloon and secure with silk ties (FIGURE 29.1)
![]() Placement and Gastric Balloon Inflation
Placement and Gastric Balloon Inflation
![]() Lubricate the gastroesophageal balloon tamponade (GEBT). Insert orogastrically so that the 50-cm mark aligns with the patient’s lip. Can insert nasally; however, the oral route is preferred (FIGURE 29.2).
Lubricate the gastroesophageal balloon tamponade (GEBT). Insert orogastrically so that the 50-cm mark aligns with the patient’s lip. Can insert nasally; however, the oral route is preferred (FIGURE 29.2).
![]() Confirm placement via air insufflation through gastric port and auscultation for gastric sounds
Confirm placement via air insufflation through gastric port and auscultation for gastric sounds
![]() Connect gastric port to 60 to 120 mm Hg intermittent suction. Inflate the gastric balloon with 50 cc of air.
Connect gastric port to 60 to 120 mm Hg intermittent suction. Inflate the gastric balloon with 50 cc of air.
![]() Confirm with chest x-ray that the inflated balloon is in the stomach
Confirm with chest x-ray that the inflated balloon is in the stomach
![]() Inflate additional 200 cc of air into gastric balloon, for a total of 250 cc of air
Inflate additional 200 cc of air into gastric balloon, for a total of 250 cc of air
![]() Affix padded Kelly clamp to gastric balloon port
Affix padded Kelly clamp to gastric balloon port
![]() Traction
Traction
![]() The proximal end of the GEBT needs to be secured with traction
The proximal end of the GEBT needs to be secured with traction
![]() Attach Kerlix distal to SB tube ports by creating a slip knot. Secure the opposing end to 1-L NS bag (or similar weight).
Attach Kerlix distal to SB tube ports by creating a slip knot. Secure the opposing end to 1-L NS bag (or similar weight).
![]() Hang Kerlix over the IV pole, allowing the 1-L NS bag to hang freely, applying traction to the SB tube
Hang Kerlix over the IV pole, allowing the 1-L NS bag to hang freely, applying traction to the SB tube
![]() Esophageal Balloon Inflation
Esophageal Balloon Inflation
![]() Connect sphygmomanometer to the three-way stopcock on esophageal balloon port
Connect sphygmomanometer to the three-way stopcock on esophageal balloon port
![]() Inflate the esophageal balloon to 30 to 45 mm Hg (typically 50–70 cc air), using lowest pressure necessary
Inflate the esophageal balloon to 30 to 45 mm Hg (typically 50–70 cc air), using lowest pressure necessary
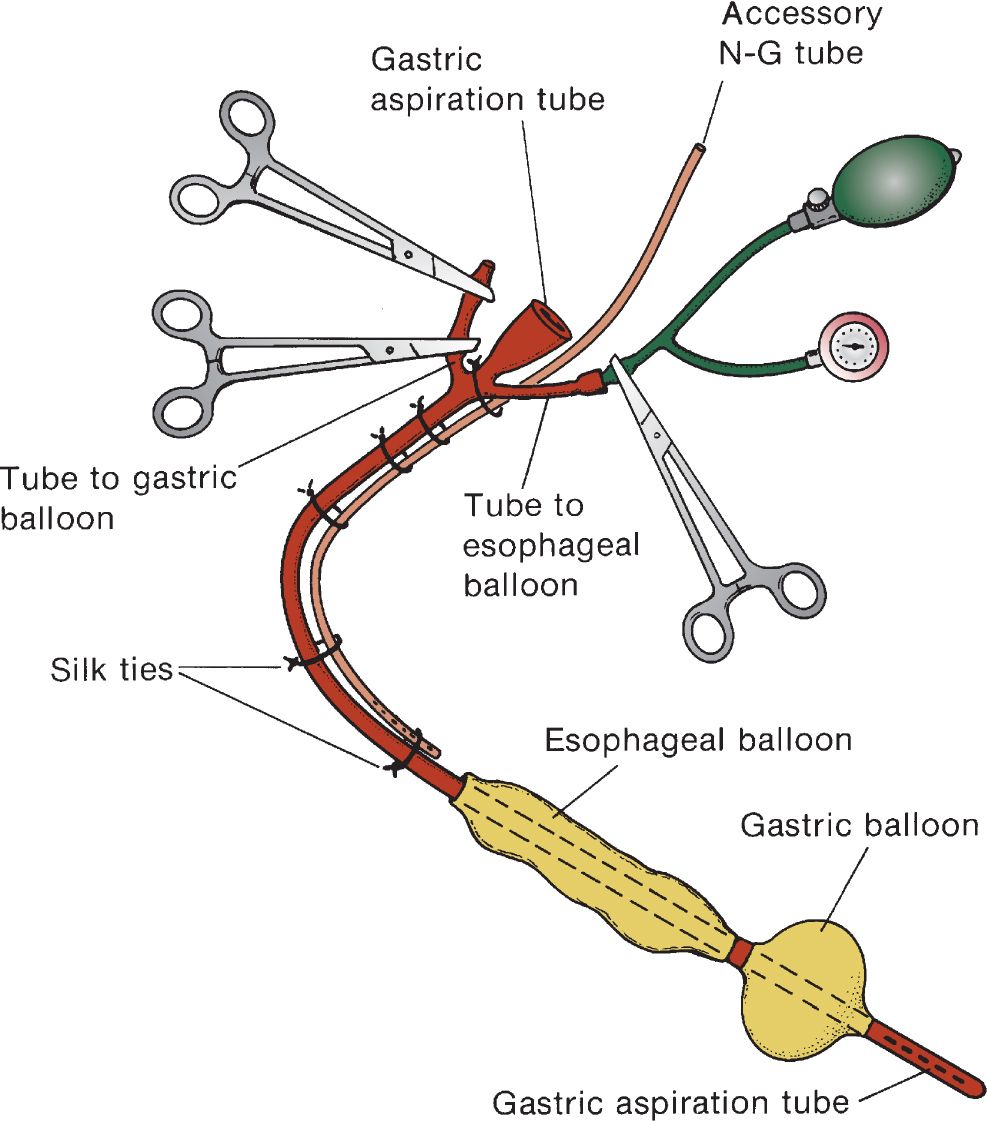
FIGURE 29.1 Modified Sengstaken–Blakemore tube. Also available is the Minnesota tube, which has a built-in esophageal port. (Reused with permission from Yamada T. Textbook of Gastroenterology. 4th ed. Vol 1. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:707.)

Full access? Get Clinical Tree


