47-year-old man with polytrauma. AP radiograph of the right distal tibia and fibula. There is a comminuted fracture of the tibia that extends from the joint line of the ankle proximally into the shaft. There is an accompanying distal fibular shaft fracture.


Sagittal (B) and coronal (C) CT of the right distal tibia and fibula. There is severe comminution and the involvement of the articular surface and distal metaphysis of the tibia.

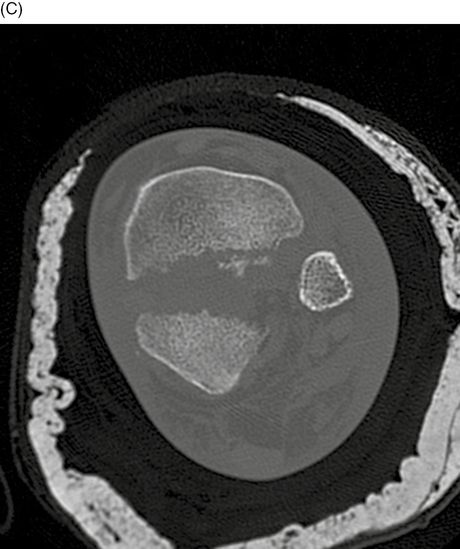
Axial CT at the right distal tibia and fibula, just superior to the tibial plafond. The characteristic fracture pattern is present, with anterior, posterior, and medial major fragments, and central comminution. This injury is called a pilon fracture, and is the result of severe axial compression that is transmitted through the foot and ankle joint to the distal tibia [1–2]. A common circumstance for this fracture is an automobile crash where the feet are braced against the floorboard at the moment of impact.
Case 12–2
Pilon fracture of tibia


85-year-old woman injured in a high-speed motor vehicle crash. AP (A) and lateral (B) radiographs of the left ankle. There is an intra-articular fracture of the distal tibia in the coronal plane. There is an avulsion fracture of the tip of the medial malleolus, and the medial ankle mortise is widened. There is extensive soft tissue swelling.
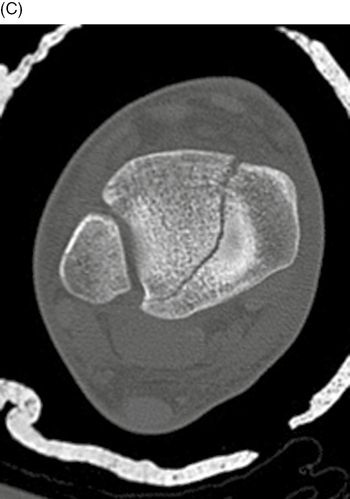
Axial CT at the left distal tibia. There is a displaced intra-articular fracture of the tibia in the coronal plane and dislocation of the distal tibio-fibular joint.
Case 12–3
Distal tibial shaft fracture


35-year-old man injured as a pedestrian struck by a car. Lateral (A) and AP (B) radiographs of the right distal tibia and fibula. There is a comminuted fracture of the distal tibial shaft with an intra-articular component extending to the ankle joint.
Axial CT of the right distal tibia. There is a mildly displaced intra-articular fracture of the tibial plafond dividing it into anterolateral and posteromedial fragments.


Sagittal (D) and coronal (E) CT of the right distal tibia. The distal intra-articular fracture does not have a step-off at the articular surface.
Case 12–4
Lateral ankle sprain



32-year-old woman who injured her ankle at the gym. AP (A), mortise (B), and lateral (C) radiographs of the left ankle. There is soft tissue swelling over the lateral malleolus, more evident when the medial and lateral sides are compared. No fracture is present. This appearance indicates a lateral ankle sprain, and usually corresponds to a tear of the anterior talofibular ligament. There is also an ankle effusion that is evident on the lateral radiograph (arrow).
Case 12–5
Lateral malleolar fracture



23-year-old woman who twisted her ankle. Lateral (A), AP (B), and mortise (C) radiographs of the right ankle. There is an oblique fracture of the distal fibula (arrow), extending from the posterior cortex inferiorly to the anterior cortex. The fracture extends to the level of the tibio-fibular syndesmosis. There is overlying soft tissue swelling. The distal fragment is only mildly displaced. This is the most common type of ankle fracture. The Danis-Weber system focuses exclusively on the level of the fibular fracture [3–5]. An ankle fracture in which the fibular fracture is entirely below the syndesmosis classified as a Weber A. If a portion of the fibular fracture extends to the level of the syndesmosis, it is a Weber B. If the fibular fracture is entirely above the syndesmosis, it is a Weber C. If there is no fibular fracture, the classification system does not apply. This case would be classified as a Weber B.
Case 12–6
Lateral malleolar fracture



30-year-old man injured his ankle playing soccer. Lateral (A), AP (B), and mortise (C) radiographs of the right ankle. There is an oblique fracture of the distal fibula (arrow) with minimal displacement. The fracture extends from the posterior cortex inferiorly to the level of the syndesmosis. The overlying soft tissues are swollen, but the ankle mortise appears intact. This injury is a Weber B. Based on cadaver studies, Lauge-Hansen [6–10] described four mechanisms for ankle fractures. Each mechanism is a combination of foot position and direction of force, with multiple stages of severity: Supination-Adduction (S-A), Supination External Rotation (S-ER), Pronation-Abduction (P-A), and Pronation-External Rotation (P-ER). The most common stage is S-ER, with four stages of severity: anterior tibiofibular ligament tear (Stage 1), oblique fracture of the lateral malleolus extending distally to the level of the plafond (anteroinferior to posterosuperior; Stage 2), posterior malleolar avulsion fracture or posterior tibial-fibular ligament tear (Stage 3), and transverse medial malleolar avulsion fracture or deltoid ligament rupture (classic trimalleolar; Stage 4). This case fits the S-ER mechanism.
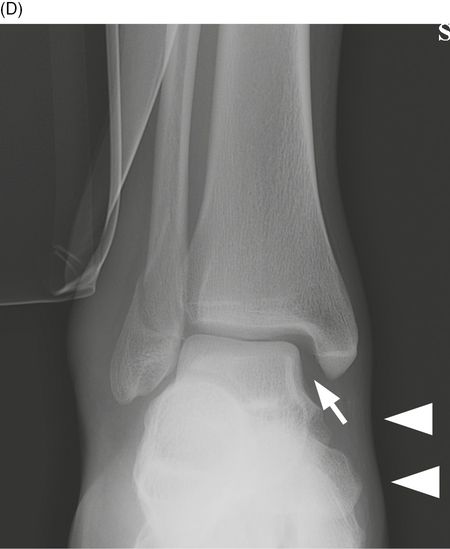
AP passive stress radiograph of the right ankle. The passive stress radiograph is obtained by laying the patient on the injured side and placing a cushion underneath the leg. The foot and ankle dangle over the end of the cushion, and the weight of the foot provides passive stress on the fracture site. The arrowheads indicate the direction of the stress. A horizontal x-ray beam is used to expose the radiograph. There is lateral displacement of the distal fibula fragment, lateral shift of the talus within the ankle mortise, and widening of the space (arrow) between the talus and the medial malleolus. This widening indicates that the deltoid ligament, which attaches the medial malleolus to the talus and calcaneus, is torn, and that the ankle is unstable. This case fits Lauge-Hansen S-ER, Stage 4.
Case 12–7
Distal fibular shaft fracture



50-year-old woman with ground-level fall. AP (A), mortise (B), and lateral (C) radiographs of the left ankle. There is a laterally displaced oblique fracture of the distal fibular shaft that is entirely above the level of the distal tibio-fibular syndesmosis. The syndesmosis itself is widened (arrowhead). There is an abnormally large space between the medial malleolus and the talus (long arrow), consistent with deltoid ligament disruption, and the talus is shifted laterally with respect to the tibia. This fracture would be classified as a Weber C. Under the Lauge-Hansen system, this injury would be classified as Pronation-External Rotation (P-ER), which has the following stages: medial malleolar fracture or deltoid ligament rupture (Stage 1), anterior tibio-fibular ligament disruption (Stage 2), fibular fracture above syndesmosis (Stage 3), and posterior malleolar fracture or posterior tibio-fibular ligament disruption (Stage 4). In this case, the displacement of the talus and lateral malleolus indicate that the posterior tibio-fibular ligament has been disrupted, making this P-ER, Stage 4.
Related posts:







Full access? Get Clinical Tree


