Forensic Aspects of Motor Vehicle Trauma
William S. Smock
Motor-vehicle–related trauma claimed 42,636 lives and injured more than 2.7 million people in the United States in 2004 (1). The majority of these victims sought care and treatment in emergency departments and trauma centers. In many cases, law enforcement officials investigating these incidents had forensic questions such as those listed below for the emergency physicians and nurses caring for the injured:
“Doc, any idea which one was the driver? They were both ejected.”
“Nurse, was any evidence from the hit-and-run vehicle transferred to the victim’s clothes?”
“What do you think took the lady’s hand off? There wasn’t much damage to the car.”
“Doc, any chance the pedestrian was already lying in the roadway when he was hit?”
The forensically trained emergency care provider should be able to answer these mysteries.
There are potential legal (criminal and civil) implications and consequences for these victims if an emergency physician or nurse fails to adequately document their injuries and preserve forensic evidence. Even injuries that seem superficial and not life threatening may hold the key to answering some of the investigating officer’s forensic questions. Emergency care providers must be trained to provide the victim of motor vehicle trauma the same level of forensic care given to the victim of a gunshot wound, child abuse, or sexual assault (2). If, through omission or commission, we, as care givers, deny our patients access to their own short-lived “evidence,” we have committed a disservice and may be culpable.
Driver or Passenger?
The determination of a vehicle occupant’s role in a serious automobile collision is an important medicolegal task. If the vehicle’s occupant is pinned with his seat belt on or behind the steering wheel, the determination is easy. If the vehicle’s occupants are ejected from the vehicle, the determination is much more difficult. Many impaired drivers will lie about their role, claiming to be a “passenger” to avoid liability. Evidence, some of which is short-lived, that could aid in making the determination of driver or passenger can be very fragile. There is a risk of altering or destroying evidence during the delivery of emergency treatment. The collection of material evidence should be a routine part of emergency medical care (2,3,4). Pattern injuries, that is, injuries that can be matched to an object, are themselves one type of “evidence.” Although not life threatening, seat-belt and air-bag abrasions, steering wheel contusions, and dicing lacerations may be critical factors in determining an occupant’s position in the vehicle at the time of the incident. As such, they must be recognized and documented.
In the isolation of the emergency department, the emergency physician or nurse should never render an opinion as to an occupant’s position (2,3,4). Investigating professionals can offer such
an opinion when the incident scene, the vehicle itself, and the occupants have been thoroughly assessed and analyzed. Similarly, allegations of criminal and/or civil liability must be based solely on the tangible physical evidence collected from the vehicle, its occupants, and the crash scene. Emergency personnel must refrain from rendering an opinion, as their insight is only one-third of the puzzle. Heath care providers must not set themselves up for the legal sequelae or embarrassment of rendering an opinion based on such a limited foundation. However, the medical component is fully a third of the investigative puzzle. Without this information, the incident reconstructionists will be challenged to arrive at an accurate opinion. Other potential roadblocks to determining the role of an occupant are listed below (4):
an opinion when the incident scene, the vehicle itself, and the occupants have been thoroughly assessed and analyzed. Similarly, allegations of criminal and/or civil liability must be based solely on the tangible physical evidence collected from the vehicle, its occupants, and the crash scene. Emergency personnel must refrain from rendering an opinion, as their insight is only one-third of the puzzle. Heath care providers must not set themselves up for the legal sequelae or embarrassment of rendering an opinion based on such a limited foundation. However, the medical component is fully a third of the investigative puzzle. Without this information, the incident reconstructionists will be challenged to arrive at an accurate opinion. Other potential roadblocks to determining the role of an occupant are listed below (4):
Occupants are removed from vehicles by well-meaning bystanders, whose statements and observations are not recorded by the investigating agencies.
Physical evidence of occupant movement within the vehicle and trace evidence of occupant and vehicle interaction are not recognized, collected, and documented.
Other occupants’ injuries, including pattern injuries, are not described in the medical record or photographically documented in the emergency department.
Evidence standards (clothing, shoes) and biological standards (hair and blood) are not collected from all occupants.
An autopsy is not conducted on the deceased occupant(s).
Substandard analysis of the crash scene prohibits accurate reconstruction of the vehicle dynamics.
Vehicle components found at the crash scene are haphazardly thrown back into the vehicles, resulting in the possibility or supposition of cross-contamination.
Inadequate resources are committed to the evaluation of the incident.
An assumption is made that the owner of the vehicle is always the driver.
The vehicle is not preserved or is left exposed to the environment, which may lead to degradation, destruction, or loss of trace evidence.
Pattern Injuries
Matching pattern injuries with interior vehicle components will reveal an occupant’s position during a portion of the vehicle’s collision sequence (2,3,4,5). Common pattern injuries include contusions, abrasions, and lacerations from seat belts, steering wheels, air bags, air-bag module covers, window cranks, radio knobs, door latches, dashboard components, and front and side window glass (Figs.5.1, 5.2, and 5.3) (2,3,4,6). An occupant’s movement and subsequent contact with a vehicle’s components are dictated by the forces applied to the vehicle through its interaction with the environment. Vehicle occupants, restrained or unrestrained, will initially move toward the primary area of impact (3,4). This movement within the vehicle, called occupant kinematics Occupant kinematics, is described as a motion parallel to and opposite from the direction of the force developed by the impacting object (3,4). Applying the principles of occupant kinematics will predict in what direction a particular occupant will move and therefore what interior component will be struck.
 Fig. 5.1 Impact with the steering and seat belt resulted in a pattern imprint on the driver’s anterior chest. This pattern injury assists in the determination of occupant role |
 Fig. 5.2 Driver or passenger? A seat-belt abrasion Seat-belt abrasion over the left neck and chest indicated the patient was restrained. The abrasions could have resulted from loading the center, the left rear, or the driver’s restraint but they do not prove she was the driver |
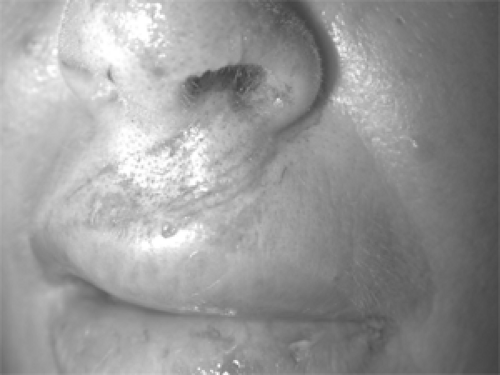 Fig. 5.3 An air-bag fabric imprint and abrasions to the upper lip |
A deploying air bag may induce unique pattern abrasions on the face, cornea, forearms, or other exposed tissue. Pattern lacerations, specific fracture patterns, and amputations are seen when the deploying air-bag module cover impacts the hand, forearm, or feet (Fig 5.3, 5.4, and 5.5 (6,7). The correlation of these injuries with the driver or passenger air-bag system is very helpful in assessing an occupant’s role (6,7,8).
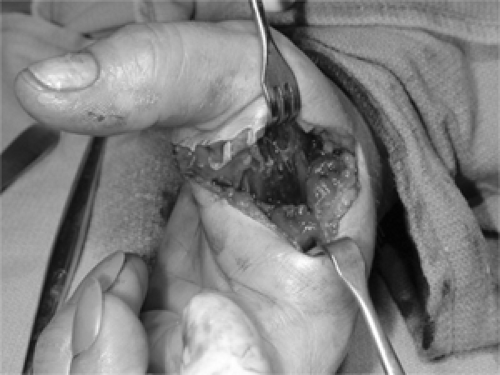 Fig. 5.4 Partial thumb amputation Partial thumb amputation from impact with a deploying driver’s air bag. Blood on the driver’s air bag was matched to the reported “passenger.” |
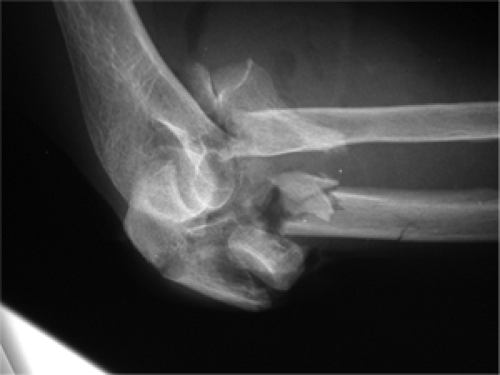 Fig. 5.5 An open comminuted elbow fracture from impact with a deploying passenger air bag. Blood and DNA on the air bag confirmed the “passenger” was in the right front passenger seat |
Both laminated (windshields) and tempered (side and rear windows) glass produce unique pattern injuries. The windshield is composed of two layers of glass laminated together with a thin layer of clear plastic sandwiched between. Laminated glass breaks into shards on impact (Fig 5.6A, B). Tempered, or “safety,” glass is a single layer of glass that breaks into small cubes when fractured. Shattered
tempered glass from side and rear windows imparts a “dicing” pattern to the skin (Fig 5.7), whereas shattered laminated windshield glass causes linear incised wounds (Fig 5.6B).
tempered glass from side and rear windows imparts a “dicing” pattern to the skin (Fig 5.7), whereas shattered laminated windshield glass causes linear incised wounds (Fig 5.6B).
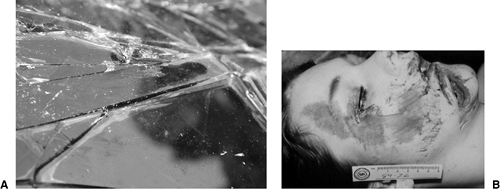 Fig. 5.6 The laminated windshield glass fractures into shards. Blood and hair are easily deposited during contact. B: Contact with windshield glass results in linear incised wounds. |
 Fig. 5.7 Sliding contact with tempered glass, which is found in side and rear windows, results in “dicing” lacerations and “cube-like” wounds. |
Trace Evidence
In the emergency department, an examination of clothing, shoes, and biologic standards (hair and blood) will assist in determining an occupant’s role (2,3,4,5,8). Examination of the soles of leather shoes may reveal the imprint of the gas or brake pedal (Fig 5.8). Preservation of clothing from all occupants permits comparison of clothing fibers with those fibers transferred to vehicle components during the collision (2,3,4,5,8). Imprints of fabric may also be transferred to components within the vehicle, including the steering wheel (Fig 5.9). Contact with the windshield often transfers hair and tissue to the glass. Glass collected from within a patient’s wound can be matched with a particular window within the vehicle. Clothes, shoes, and other evidence should be collected and maintained if the role of the occupant in the collision is unclear.
 Fig. 5.8 An imprint of the brake or accelerator pedal can be transferred to leather soles. Examination of shoes can assist in the determination of an occupant’s role. |
 Fig. 5.9 Forceful impact of clothing, impact of clothing against vehicle components can impart a fabric transfer. The comparison of the fabric weave from the imprint on the steering wheel assisted in determining which occupant was the driver |
Air bags and their module covers are also a tremendous source of trace evidence. Blood, hair, makeup, and skin are easily transferred to the air-bag’s canvas surface during impact (Fig 5.10 and (Fig 5.11)) (6,7,8). The module cover will also yield transferred blood, tissue, and imprints from fabric or the soles of shoes (Fig 5.12 and (Fig 5.13).
Related posts:





Full access? Get Clinical Tree


